

Appropriate and Inappropriate Implantable Cardioverter Defibrillators Therapies in Arrhythmogenic Right Ventricular Cardiomyopathy/Dysplasia Patients
- PMID: 30116448
- PMCID: PMC6089463
- DOI: 10.14740/cr734w
Appropriate and Inappropriate Implantable Cardioverter Defibrillators Therapies in Arrhythmogenic Right Ventricular Cardiomyopathy/Dysplasia Patients
Abstract
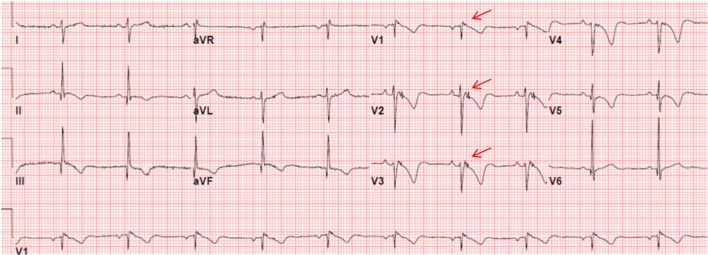
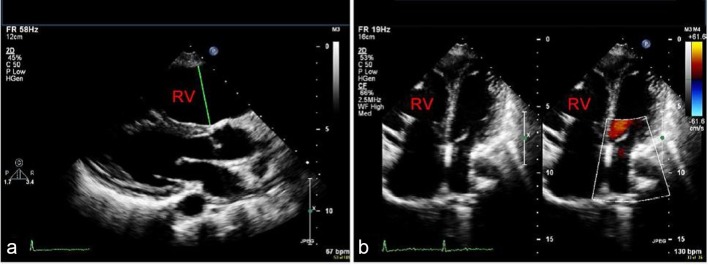
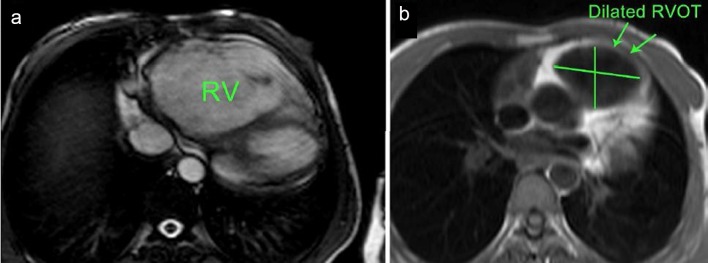
Background: Arrhythmogenic right ventricular cardiomyopathy/dysplasia (ARVC/D) is an inherited cardiomyopathy characterized histologically by the replacement of ventricular myocardium with fibrous and fatty tissue, and clinically by ventricular tachycardia arrhythmias primarily of right ventricular (RV) origin. Implantable cardioverter defibrillator (ICD) is the only proven therapy to reduce mortality in ARVC/D patients. However, it has the risk of inappropriate anti-tachycardia pacing (ATP) or shocks. This study aimed to assess the occurrence of appropriate and inappropriate ICD therapies in ARVC/D patients who underwent ICD implantation in a single Cardiac Centre.
Methods: Retrospective analysis of the data of patients with the diagnosis of ARVC/D based on the 2010 revised Task Force Criteria, who underwent ICD implantation in the Heart Centre, at King Faisal Specialist Hospital and Research Center (KFSH&RC), Riyadh between January 1997 and May 2016. The clinical data and information about appropriate and inappropriate ICD therapies were obtained from medical records with the review of the available intra-cardiac electrograms (EGMs).
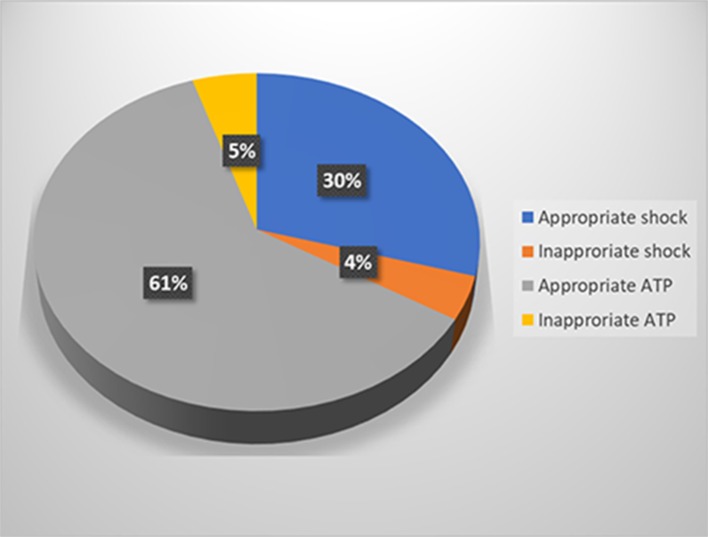
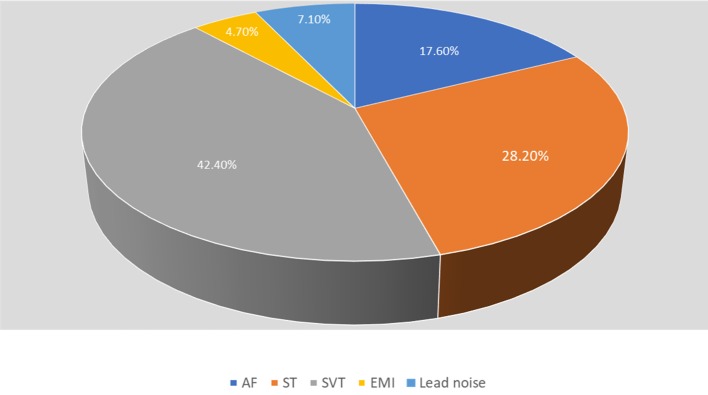
Results: Twenty-two ARVC/D patients with ICD implantation (20 males (91%), mean age at ICD implantation: 32 ± 14 years). ICD was implanted for secondary prevention of sudden cardiac death (SCD) in 15 patients (68.2%), and for primary prevention in 7 patients (31.8%). At mean follow-up of 9.4 ± 4.8 years, 11 patients (50%) had appropriate ICD therapies, and five patients (22.7%) had inappropriate ICD therapies. Out of 950 ICD therapies, 865 (91%) were appropriate (586 episodes of VT/VF treated with ATP (61.3%), and 279 episodes treated with shocks (29.37%)) and 85 (9.4%) were inappropriate (45 episodes treated with ATP (4.73%), and 40 treated with shocks (4.21%)).
Conclusion: ARVC/D patients are at risk of VT/VF arrhythmias. ICD therapy is the only proven life-saving therapy in those patients. Most of ICD therapies in our patient's population are appropriate, and ATP therapy is effective in terminating most of VT episodes. Although we do not have any patient with subcutaneous ICD, the high success rate of ATP suggests that transvenous ICD would be more appropriate in ARVC/D patients.
Keywords: Anti-tachycardia pacing; Arrhythmogenic right ventricular cardiomyopathy; Implantable cardioverter defibrillator; Shocks.
Conflict of interest statement
The authors declare no conflict of interest related to this article.
Figures

Similar articles
-
Arrhythmogenic right ventricular cardiomyopathy/dysplasia in Saudi Arabia: a single-center experience with long-term follow-up.Ann Saudi Med. 2014 Sep-Oct;34(5):415-26. doi: 10.5144/0256-4947.2014.415. Ann Saudi Med. 2014. PMID: 25827699 Free PMC article.
-
Subcutaneous Implantable Cardioverter-Defibrillator in Patients With Arrhythmogenic Right Ventricular Cardiomyopathy/Dysplasia: A Transatlantic Experience.J Am Heart Assoc. 2018 Nov 6;7(21):e008782. doi: 10.1161/JAHA.118.008782. J Am Heart Assoc. 2018. PMID: 30608223 Free PMC article.
-
Right ventricular function is a predictor for sustained ventricular tachycardia requiring anti-tachycardic pacing in arrhythmogenic ventricular cardiomyopathy: insight into transvenous vs. subcutaneous implantable cardioverter defibrillator insertion.Europace. 2023 May 19;25(5):euad073. doi: 10.1093/europace/euad073. Europace. 2023. PMID: 37213071 Free PMC article.
-
Implantable cardioverter defibrillators in arrhythmogenic right ventricular dysplasia/cardiomyopathy: patient outcomes, incidence of appropriate and inappropriate interventions, and complications.Circ Arrhythm Electrophysiol. 2013 Jun;6(3):562-8. doi: 10.1161/CIRCEP.113.000392. Epub 2013 May 14. Circ Arrhythm Electrophysiol. 2013. PMID: 23673907 Review.
-
Radiofrequency Ablation in Arrhythmogenic Right Ventricular Cardiomyopathy (ARVC).Curr Cardiol Rep. 2017 Sep;19(9):82. doi: 10.1007/s11886-017-0893-3. Curr Cardiol Rep. 2017. PMID: 28779285 Review.
Cited by
-
The Challenges of Diagnosis and Treatment of Arrhythmogenic Cardiomyopathy: Are We there yet?Rev Cardiovasc Med. 2022 Aug 15;23(8):283. doi: 10.31083/j.rcm2308283. eCollection 2022 Aug. Rev Cardiovasc Med. 2022. PMID: 39076647 Free PMC article.
-
Ventricular arrhythmia management in patients with genetic cardiomyopathies.Heart Rhythm O2. 2021 Dec 17;2(6Part B):819-831. doi: 10.1016/j.hroo.2021.10.009. eCollection 2021 Dec. Heart Rhythm O2. 2021. PMID: 34988533 Free PMC article.
-
A Low Critical Event Rate Despite a High Abnormal Event Rate in Patients with Cardiac Implantable Electric Devices Followed Up by Remote Monitoring.Intern Med. 2019 Aug 15;58(16):2333-2340. doi: 10.2169/internalmedicine.1905-18. Epub 2019 May 22. Intern Med. 2019. PMID: 31118368 Free PMC article.
-
Inappropriate defibrillator shock due to fragmented potentials derived from an extensively diseased right ventricle in a patient with arrhythmogenic right ventricular cardiomyopathy.HeartRhythm Case Rep. 2022 Jul 19;8(10):666-670. doi: 10.1016/j.hrcr.2022.07.009. eCollection 2022 Oct. HeartRhythm Case Rep. 2022. PMID: 36310728 Free PMC article. No abstract available.
References
-
- Corrado D, Basso C, Thiene G, McKenna WJ, Davies MJ, Fontaliran F, Nava A. et al. Spectrum of clinicopathologic manifestations of arrhythmogenic right ventricular cardiomyopathy/dysplasia: a multicenter study. J Am Coll Cardiol. 1997;30(6):1512–1520. doi: 10.1016/S0735-1097(97)00332-X. - DOI - PubMed
-
- McKenna WJ, Thiene G, Nava A, Fontaliran F, Blomstrom-Lundqvist C, Fontaine G, Camerini F. Diagnosis of arrhythmogenic right ventricular dysplasia/cardiomyopathy. Task Force of the Working Group Myocardial and Pericardial Disease of the European Society of Cardiology and of the Scientific Council on Cardiomyopathies of the International Society and Federation of Cardiology. Br Heart J. 1994;71(3):215–218. doi: 10.1136/hrt.71.3.215. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources