

A multi-center nested case-control study on hospitalization costs and length of stay due to healthcare-associated infection
- PMID: 30116526
- PMCID: PMC6085640
- DOI: 10.1186/s13756-018-0386-1
A multi-center nested case-control study on hospitalization costs and length of stay due to healthcare-associated infection
Abstract
Background: In 2018, the Chinese government demanded nationwide implementation of medical insurance payment methods based on Single-Disease Payment (SDP), but during the operation process the medical insurance system did not fully consider the extra economic burden caused by healthcare-associated infection (HAI). HAIs can prolong the length of stay and increase the hospitalization costs, but only a few studies have been conducted in Sichuan province, China. We evaluated the hospitalization costs and length of stay due to HAI in Sichuan province based on the prevalence survey, and provided data reference for China's medical insurance reform.
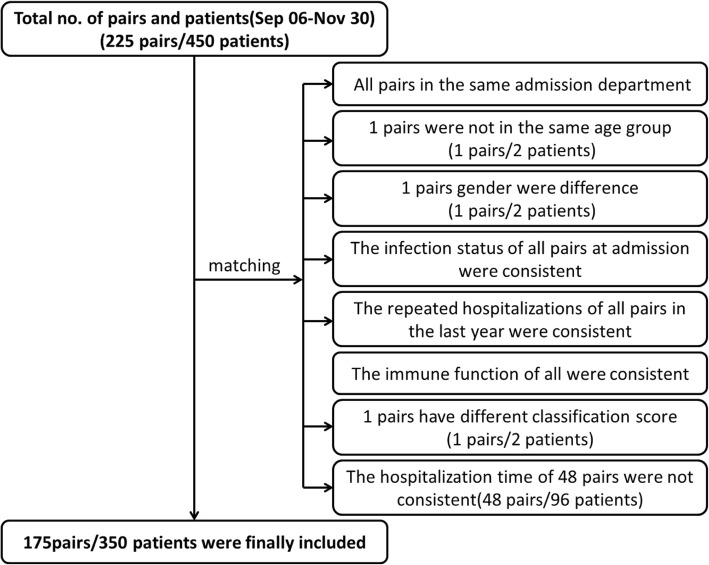
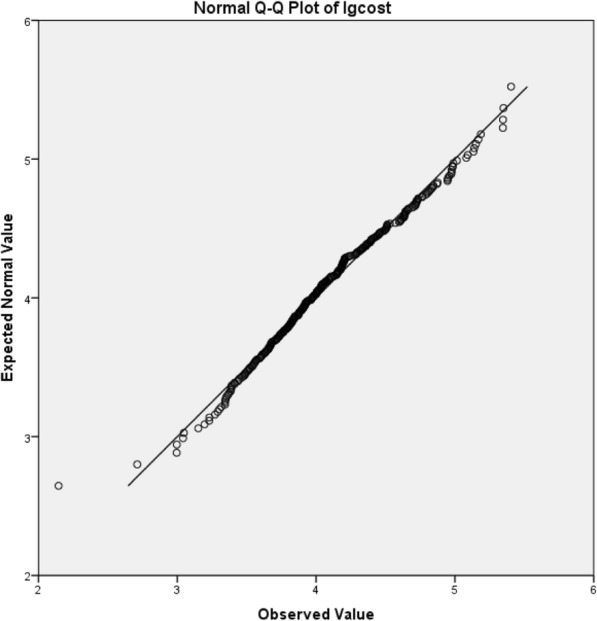
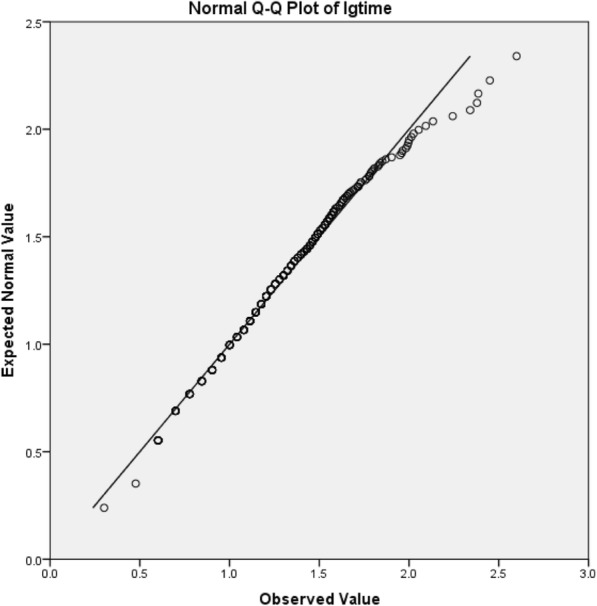
Methods: In the hospitals surveyed on the prevalence of HAI, a multi-center nested case-control study was performed by a paired method. The study period was from 6 September 2016 to 30 November 2016. Binary outcomes were tested using χ2 test, continuous outcomes were tested using Wilcoxon matched-pairs signed rank test, intra-group comparisons were tested using multiple linear regression analysis.
Results: A total of 225 pairs/450 patients were selected in 51 hospitals, and 170 pairs/350 patients were successfully matched. The case fatality rate was 5.14% for the HAIs patients and 3.43% for non-HAs patients, there was no significant difference (χ2 = 0.627, P = 0.429); the median length of stay in patients with HAIs was 21 days, longer than that of patients with non-HAI 16 days, the median of the difference between matched-pairs was 5 days, the difference was statistically significant (Z = 4.896, P = 0.000). The median hospitalization costs of patients with HAI were €1732.83, higher than that of patients with non-HAI €1095.29, the median of the difference between matched-pairs were €431.34, the difference was statistically significant (Z = 6.413, P = 0.000). Multiple linear regression results showed that HAIs at different sites have caused different economic burdens, but in different economic regions, the difference was not statistically significant.
Conclusions: In Sichuan, the hospitalization costs and length of stay caused by HAI should be given special attention in the current medical insurance reform. The proportion and scope of medical payment for patients with HAI at different sites should be different. Efforts need to be taken to incentivize reduction of HAI rates which will reduce hospitalization costs and length of stay.
Keywords: Healthcare-associated infections; Hospitalization costs; Length of stay; Multi-center; Nested case-control study.
Conflict of interest statement
Not applicable. Not applicable. The authors declare that they have no competing interests. Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Office of the Sichuan Provincial People's Government. Notice on Printing and Distributing the Implementation Plan for Further Deepening the Reform of Payment Methods for Basic Medical Insurance. Available from:http://www.sc.gov.cn/10462/12771/2018/1/8/10442346.shtml(2018). Accessed 26 July 2018.
-
- Di X. The development of specific disease payment and its key issues of management. Chinese Health Resources. 2018;21:27–31.
-
- Zhi-jian LIU. Study on the Effect of New Health Payment Scheme on Medical Costs. D. University of Science and Technology of China. 2017.
-
- Guo C, Liu YH, Tian DS. Statistical research on direct economic loss due to nosocomial infections. Chinese Journal of Nosocomiology. 2012;22(8):1651–1653.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
