

Development of a diagnostic system for detection of specific antibodies and antigens against Middle East respiratory syndrome coronavirus
- PMID: 30117617
- PMCID: PMC7168444
- DOI: 10.1111/1348-0421.12643
Development of a diagnostic system for detection of specific antibodies and antigens against Middle East respiratory syndrome coronavirus
Abstract
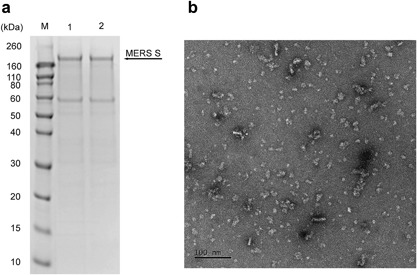
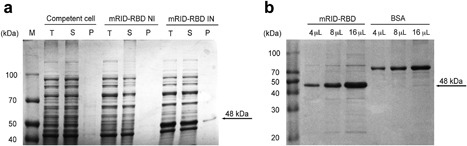
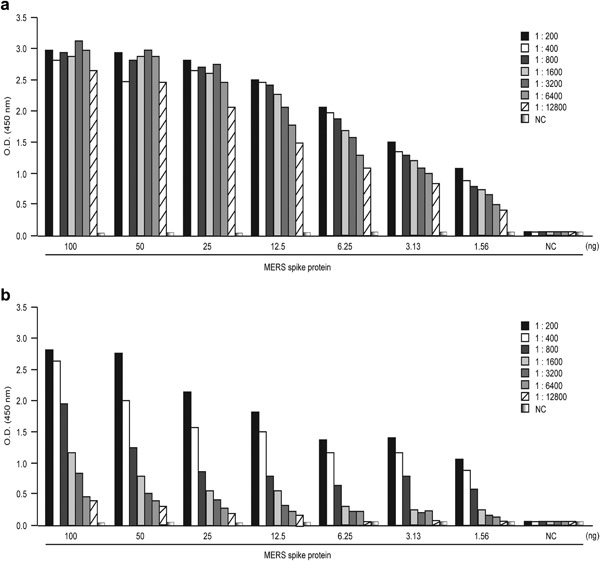
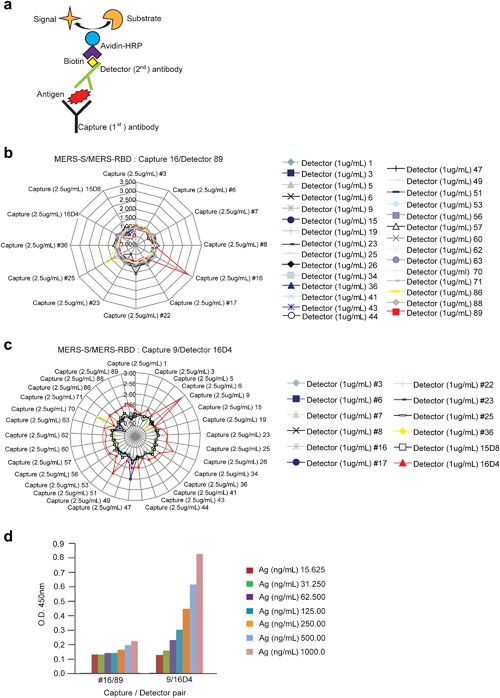
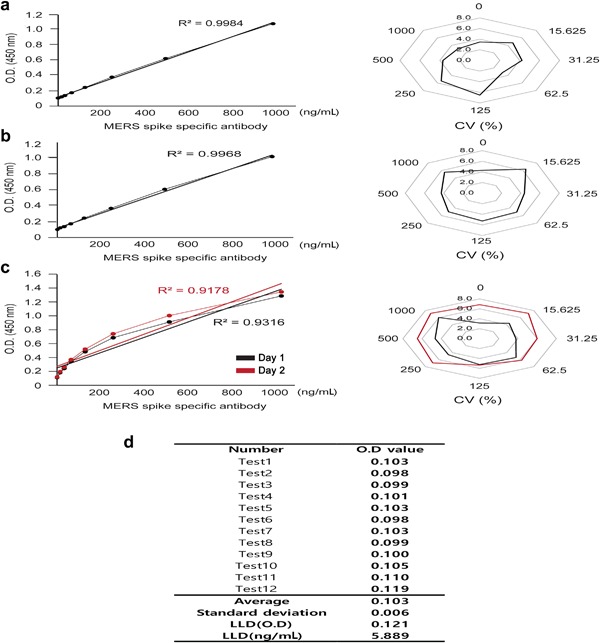
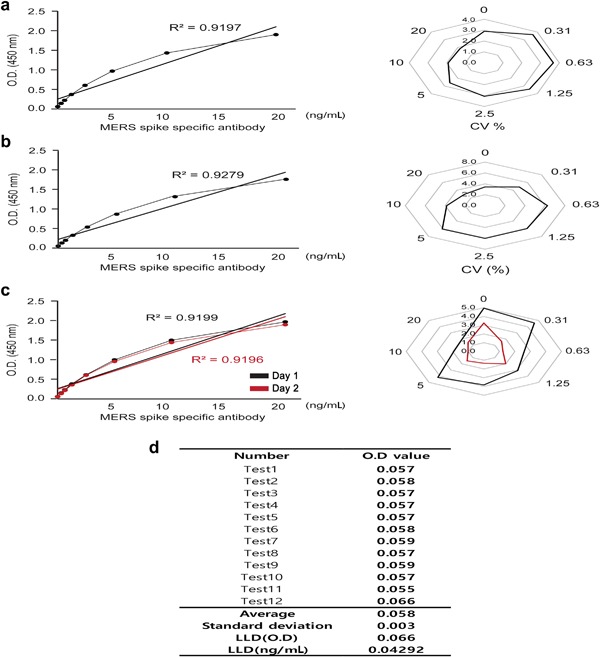
Middle East respiratory syndrome coronavirus (MERS-CoV) is a single-stranded RNA virus that causes severe respiratory disease in humans with a high fatality rate. Binding of the receptor binding domain (RBD) of the spike (S) glycoprotein to dipeptidyl peptidase 4 is the critical step in MERS-CoV infection of a host cell. No vaccines or clinically applicable treatments are currently available for MERS-CoV. Therefore, rapid diagnosis is important for improving patient outcomes through prompt treatment and protection against viral outbreaks. In this study, the aim was to establish two ELISA systems for detecting antigens and antibodies against MERS-CoV. Using a recombinant full-length S protein, an indirect ELISA was developed and found to detect MERS-CoV-specific antibodies in animal sera and sera of patient with MERS. Moreover, MAbs were induced with the recombinant S protein and RBD and used for sandwich ELISA to detect the MERS-CoV S protein. Neither ELISA system exhibited significant intra-assay or inter-assay variation, indicating good reproducibility. Moreover, the inter-day precision and sensitivity were adequate for use as a diagnostic kit. Thus, these ELISAs can be used clinically to diagnose MERS-CoV.
Keywords: ELISA; Middle East respiratory syndrome coronavirus; receptor binding domain; spike protein.
© 2018 The Societies and John Wiley & Sons Australia, Ltd.
Figures
Similar articles
-
Recombinant Receptor-Binding Domains of Multiple Middle East Respiratory Syndrome Coronaviruses (MERS-CoVs) Induce Cross-Neutralizing Antibodies against Divergent Human and Camel MERS-CoVs and Antibody Escape Mutants.J Virol. 2016 Dec 16;91(1):e01651-16. doi: 10.1128/JVI.01651-16. Print 2017 Jan 1. J Virol. 2016. PMID: 27795425 Free PMC article.
-
Characterization of anti-MERS-CoV antibodies against various recombinant structural antigens of MERS-CoV in an imported case in China.Emerg Microbes Infect. 2016 Nov 9;5(11):e113. doi: 10.1038/emi.2016.114. Emerg Microbes Infect. 2016. PMID: 27826140 Free PMC article.
-
A recombinant receptor-binding domain of MERS-CoV in trimeric form protects human dipeptidyl peptidase 4 (hDPP4) transgenic mice from MERS-CoV infection.Virology. 2016 Dec;499:375-382. doi: 10.1016/j.virol.2016.10.005. Epub 2016 Oct 15. Virology. 2016. PMID: 27750111 Free PMC article.
-
Antibodies and vaccines against Middle East respiratory syndrome coronavirus.Emerg Microbes Infect. 2019;8(1):841-856. doi: 10.1080/22221751.2019.1624482. Emerg Microbes Infect. 2019. PMID: 31169078 Free PMC article. Review.
-
Neutralizing Monoclonal Antibodies as Promising Therapeutics against Middle East Respiratory Syndrome Coronavirus Infection.Viruses. 2018 Nov 30;10(12):680. doi: 10.3390/v10120680. Viruses. 2018. PMID: 30513619 Free PMC article. Review.
Cited by
-
SARS-CoV, MERS-CoV and SARS-CoV-2: A Diagnostic Challenge.Measurement (Lond). 2021 Jan 15;168:108335. doi: 10.1016/j.measurement.2020.108335. Epub 2020 Aug 8. Measurement (Lond). 2021. PMID: 33519010 Free PMC article.
-
Multiepitope Proteins for the Differential Detection of IgG Antibodies against RBD of the Spike Protein and Non-RBD Regions of SARS-CoV-2.Vaccines (Basel). 2021 Sep 3;9(9):986. doi: 10.3390/vaccines9090986. Vaccines (Basel). 2021. PMID: 34579223 Free PMC article.
-
Solutions against emerging infectious and noninfectious human diseases through the application of baculovirus technologies.Appl Microbiol Biotechnol. 2021 Nov;105(21-22):8195-8226. doi: 10.1007/s00253-021-11615-1. Epub 2021 Oct 7. Appl Microbiol Biotechnol. 2021. PMID: 34618205 Free PMC article. Review.
-
A novel luciferase immunosorbent assay performs better than a commercial enzyme-linked immunosorbent assay to detect MERS-CoV specific IgG in humans and animals.Biosaf Health. 2019 Dec;1(3):134-143. doi: 10.1016/j.bsheal.2019.12.006. Epub 2019 Dec 20. Biosaf Health. 2019. PMID: 32501446 Free PMC article.
-
Current diagnostic approaches to detect two important betacoronaviruses: Middle East respiratory syndrome coronavirus (MERS-CoV) and severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2).Pathol Res Pract. 2021 Sep;225:153565. doi: 10.1016/j.prp.2021.153565. Epub 2021 Jul 24. Pathol Res Pract. 2021. PMID: 34333398 Free PMC article. Review.
References
-
- Zaki A.M., Van Boheemen S., Bestebroer T.M., Osterhaus A.D., Fouchier R.A. (2012) Isolation of a novel coronavirus from a man with pneumonia in Saudi Arabia. N Engl J Med 367: 1814–20. - PubMed
-
- Bermingham A., Chand M.A., Brown C.S., Aarons E., Tong C., Langrish C., Hoschler K., Brown K., Galiano M., Myers R., Pebody R.G., Green H.K., Boddington N.L., Gopal R., Price N., Newsholme W., Drosten C., Fouchier R.A., Zambon M. (2012) Severe respiratory illness caused by a novel coronavirus, in a patient transferred to the United Kingdom from the Middle East, September 2012. Euro Surveill 17: 20290. - PubMed
-
- Gierer S., Bertram S., Kaup F., Wrensch F., Heurich A., Kramer‐Kuhl A., Welsch K., Winkler M., Meyer B., Drosten C., Dittmer U., Von Hahn T., Simmons G., Hofmann H., Pohlmann S. (2013) The spike protein of the emerging betacoronavirus EMC uses a novel coronavirus receptor for entry, can be activated by TMPRSS2, and is targeted by neutralizing antibodies. J Virol 87: 5502–11. - PMC - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
