

Carbon dioxide dynamics in relation to neurological outcome in resuscitated out-of-hospital cardiac arrest patients: an exploratory Target Temperature Management Trial substudy
- PMID: 30119692
- PMCID: PMC6098627
- DOI: 10.1186/s13054-018-2119-5
Carbon dioxide dynamics in relation to neurological outcome in resuscitated out-of-hospital cardiac arrest patients: an exploratory Target Temperature Management Trial substudy
Abstract
Background: Dyscarbia is common in out-of-hospital cardiac arrest (OHCA) patients and its association to neurological outcome is undetermined.
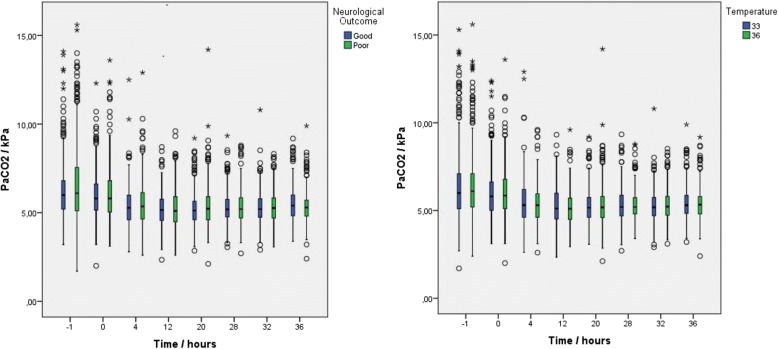
Methods: This is an exploratory post-hoc substudy of the Target Temperature Management (TTM) trial, including resuscitated OHCA patients, investigating the association between serial measurements of arterial partial carbon dioxide pressure (PaCO2) and neurological outcome at 6 months, defined by the Cerebral Performance Category (CPC) scale, dichotomized to good outcome (CPC 1 and 2) and poor outcome (CPC 3-5). The effects of hypercapnia and hypocapnia, and the time-weighted mean PaCO2 and absolute PaCO2 difference were analyzed. Additionally, the association between mild hypercapnia (6.0-7.30 kPa) and neurological outcome, its interaction with target temperature (33 °C and 36 °C), and the association between PaCO2 and peak serum-Tau were evaluated.
Results: Of the 939 patients in the TTM trial, 869 were eligible for analysis. Ninety-six percent of patients were exposed to hypocapnia or hypercapnia. None of the analyses indicated a statistical significant association between PaCO2 and neurological outcome (P = 0.13-0.96). Mild hypercapnia was not associated with neurological outcome (P = 0.78) and there was no statistically significant interaction with target temperature (Pinteraction = 0.95). There was no association between PaCO2 and peak serum-Tau levels 48 or 72 h after return of spontaneous circulation (ROSC).
Conclusions: Dyscarbia is common after ROSC. No statistically significant association between PaCO2 in the post-cardiac arrest phase and neurological outcome at 6 months after cardiac arrest was detected. There was no significant interaction between mild hypercapnia and temperature in relation to neurological outcome.
Keywords: Biomarker; Carbon dioxide partial pressure; Cerebral performance; Out-of-hospital cardiac arrest; Serum Tau.
Conflict of interest statement
Ethics approval and consent to participate
The TTM trial protocol was approved by ethics committees in the following institutions: St George Hospital, Sydney, Australia; North Shore Hospital, Sydney, Australia; Liverpool Hospital, Sydney, Australia; The George Institute of Global Health, Sydney, Australia; General University Hospital in Prague, Prague, Czech Republic; The Heart Center, Copenhagen University Hospital Rigshospitalet, Copenhagen, Denmark; Ospedale Universitario di Cattinara, Trieste, Italy; Santa Maria degli Angeli Hospital, Pordenone, Italy; San Martino, Genoa, Italy; Medical Centre, Luxembourg; Amsterdam Medical Centre, Amsterdam, the Netherlands; Leeuwarden Hospital, Leeuwarden, the Netherlands; Rijnstaate Hospital, Arnhem, the Netherlands; Onze Lieuwe Vrouwe Gasthuis, Amsterdam, the Netherlands; Oslo University Hospital, Oslo, Norway; Haukeland University Hospital, Bergen, Norway; Helsingborg Hospital, Helsingborg, Sweden; Karlstad Hospital, Karlstad, Sweden; Kungälv Hospital, Kungälv, Sweden; Linköping University Hospital, Linköping, Sweden; Skåne University Hospital, Lund, Sweden; Skåne University Hospital, Malmö, Sweden; Norra Älvsborgs Län Hospital, Sweden; Vrinnevi Hospital, Norrköping, Sweden; Sahlgrenska University Hospital, Gothenburg, Sweden; Örebro University Hospital, Örebro, Sweden; Geneva University Hospital, Geneva, Switzerland; Hospital St Gallen, St Gallen, Switzerland; Hospital La Chaux de Fonds, Switzerland; University Hospital of Wales, Cardiff, UK; Royal Berkshire Hospital, Reading, UK; Royal Bournemouth Hospital, Bournemouth, UK; Guy’s and St Thomas’ NHS Trust, London, UK; St George’s Hospital, London, UK. Informed consent was waived or was obtained according to national legislation, in line with the Helsinki declaration.
Consent for publication
Not applicable.
Competing interests
HF has received lecture fees from Bard Medical and is scientific advisor at QuickCool.
MPW has attended an advisory board and educational meeting for Bard Medical. NN has received lecture fees from Bard Medical. The remaining authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures

References
-
- Mozaffarian D, Benjamin EJ, Go AS, Arnett DK, Blaha MJ, Cushman M, Das SR, de Ferranti S, Despres JP, Fullerton HJ, et al. Heart disease and stroke statistics—2016 update: a report from the American Heart Association. Circulation. 2016;133(4):e38–e360. doi: 10.1161/CIR.0000000000000350. - DOI - PubMed
-
- Adielsson A, Hollenberg J, Karlsson T, Lindqvist J, Lundin S, Silfverstolpe J, Svensson L, Herlitz J. Increase in survival and bystander CPR in out-of-hospital shockable arrhythmia: bystander CPR and female gender are predictors of improved outcome. Experiences from Sweden in an 18-year perspective. Heart. 2011;97(17):1391–1396. doi: 10.1136/hrt.2011.222711. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
