

Absolute risk and predictors of the growth of acute spontaneous intracerebral haemorrhage: a systematic review and meta-analysis of individual patient data
- PMID: 30120039
- PMCID: PMC6143589
- DOI: 10.1016/S1474-4422(18)30253-9
Absolute risk and predictors of the growth of acute spontaneous intracerebral haemorrhage: a systematic review and meta-analysis of individual patient data
Erratum in
-
Corrections.Lancet Neurol. 2018 Nov;17(11):933. doi: 10.1016/S1474-4422(18)30354-5. Epub 2018 Sep 19. Lancet Neurol. 2018. PMID: 30243862 Free PMC article. No abstract available.
Abstract
Background: Intracerebral haemorrhage growth is associated with poor clinical outcome and is a therapeutic target for improving outcome. We aimed to determine the absolute risk and predictors of intracerebral haemorrhage growth, develop and validate prediction models, and evaluate the added value of CT angiography.
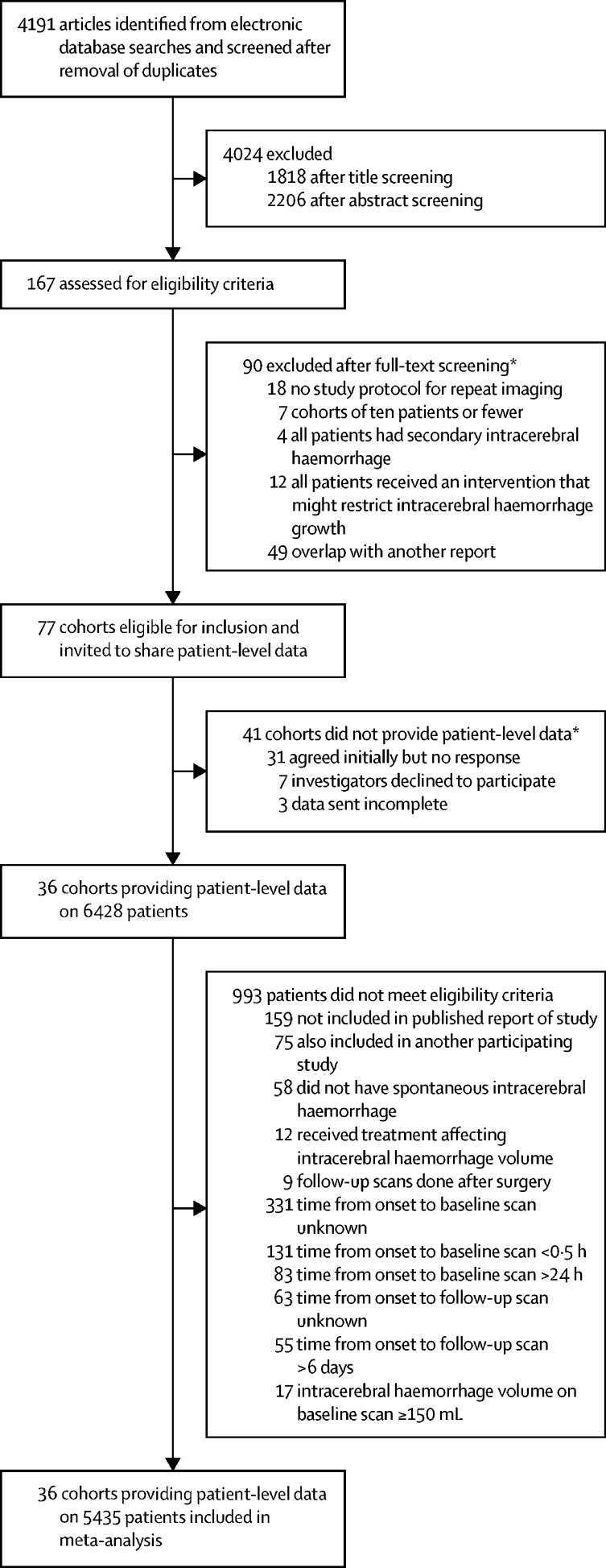
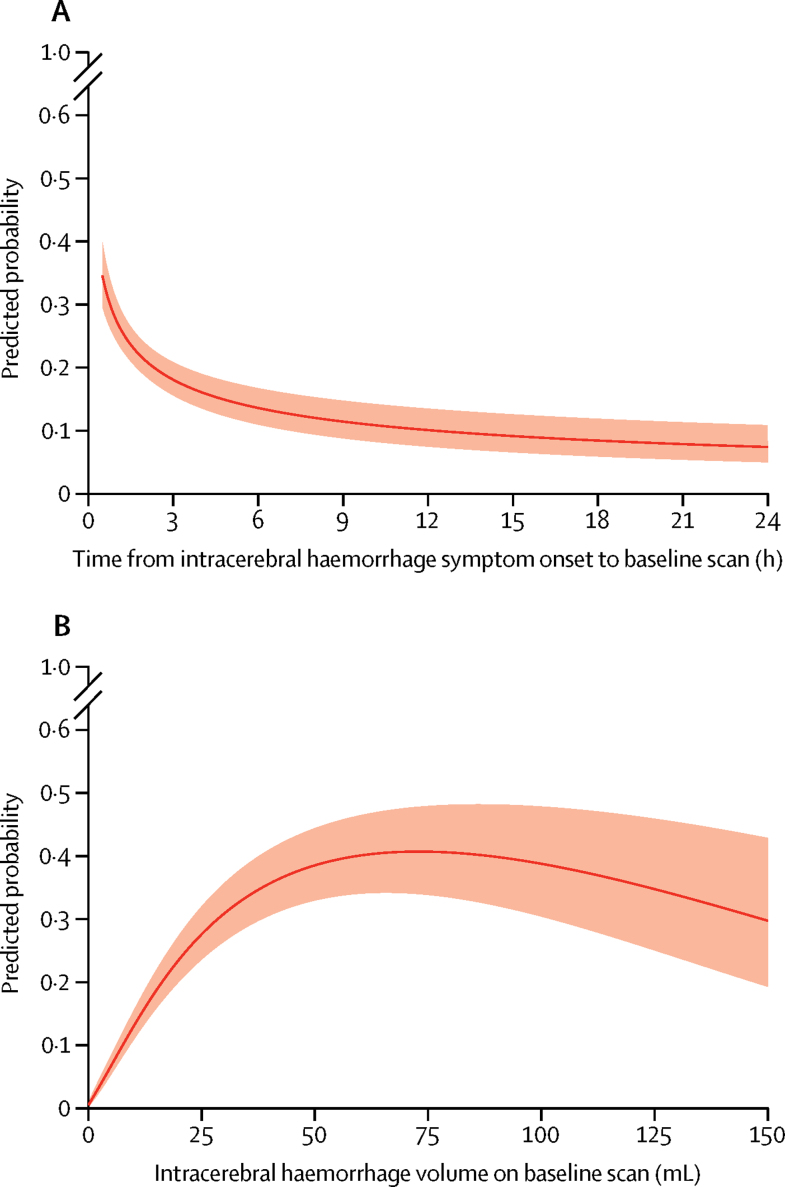
Methods: In a systematic review of OVID MEDLINE-with additional hand-searching of relevant studies' bibliographies- from Jan 1, 1970, to Dec 31, 2015, we identified observational cohorts and randomised trials with repeat scanning protocols that included at least ten patients with acute intracerebral haemorrhage. We sought individual patient-level data from corresponding authors for patients aged 18 years or older with data available from brain imaging initially done 0·5-24 h and repeated fewer than 6 days after symptom onset, who had baseline intracerebral haemorrhage volume of less than 150 mL, and did not undergo acute treatment that might reduce intracerebral haemorrhage volume. We estimated the absolute risk and predictors of the primary outcome of intracerebral haemorrhage growth (defined as >6 mL increase in intracerebral haemorrhage volume on repeat imaging) using multivariable logistic regression models in development and validation cohorts in four subgroups of patients, using a hierarchical approach: patients not taking anticoagulant therapy at intracerebral haemorrhage onset (who constituted the largest subgroup), patients taking anticoagulant therapy at intracerebral haemorrhage onset, patients from cohorts that included at least some patients taking anticoagulant therapy at intracerebral haemorrhage onset, and patients for whom both information about anticoagulant therapy at intracerebral haemorrhage onset and spot sign on acute CT angiography were known.
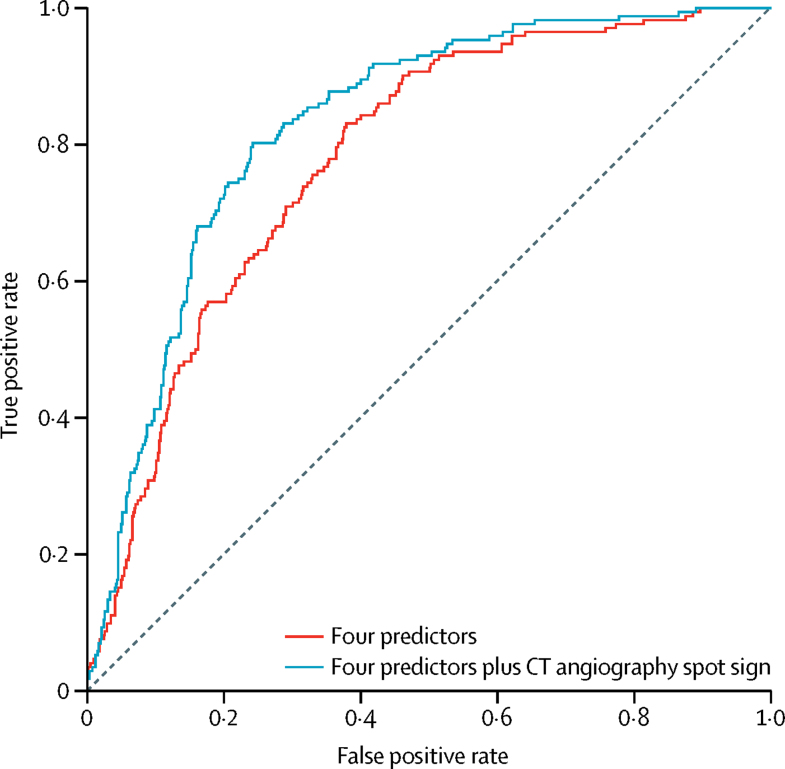
Findings: Of 4191 studies identified, 77 were eligible for inclusion. Overall, 36 (47%) cohorts provided data on 5435 eligible patients. 5076 of these patients were not taking anticoagulant therapy at symptom onset (median age 67 years, IQR 56-76), of whom 1009 (20%) had intracerebral haemorrhage growth. Multivariable models of patients with data on antiplatelet therapy use, data on anticoagulant therapy use, and assessment of CT angiography spot sign at symptom onset showed that time from symptom onset to baseline imaging (odds ratio 0·50, 95% CI 0·36-0·70; p<0·0001), intracerebral haemorrhage volume on baseline imaging (7·18, 4·46-11·60; p<0·0001), antiplatelet use (1·68, 1·06-2·66; p=0·026), and anticoagulant use (3·48, 1·96-6·16; p<0·0001) were independent predictors of intracerebral haemorrhage growth (C-index 0·78, 95% CI 0·75-0·82). Addition of CT angiography spot sign (odds ratio 4·46, 95% CI 2·95-6·75; p<0·0001) to the model increased the C-index by 0·05 (95% CI 0·03-0·07).
Interpretation: In this large patient-level meta-analysis, models using four or five predictors had acceptable to good discrimination. These models could inform the location and frequency of observations on patients in clinical practice, explain treatment effects in prior randomised trials, and guide the design of future trials.
Funding: UK Medical Research Council and British Heart Foundation.
Copyright © 2018 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Figures
Comment in
-
Risk predictors to limit neuronal loss after intracerebral haemorrhage.Lancet Neurol. 2018 Oct;17(10):834-836. doi: 10.1016/S1474-4422(18)30313-2. Epub 2018 Aug 17. Lancet Neurol. 2018. PMID: 30126645 No abstract available.
References
-
- Feigin VL, Lawes CM, Bennett DA, Barker-Collo SL, Parag V. Worldwide stroke incidence and early case fatality reported in 56 population-based studies: a systematic review. Lancet Neurol. 2009;8:355–369. - PubMed
-
- van Asch CJ, Luitse MJ, Rinkel GJ, van der Tweel I, Algra A, Klijn CJ. Incidence, case fatality, and functional outcome of intracerebral haemorrhage over time, according to age, sex, and ethnic origin: a systematic review and meta-analysis. Lancet Neurol. 2010;9:167–176. - PubMed
-
- Davis SM, Broderick J, Hennerici M. Hematoma growth is a determinant of mortality and poor outcome after intracerebral hemorrhage. Neurology. 2006;66:1175–1181. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
