

Fixed Low-Dose Triple Combination Antihypertensive Medication vs Usual Care for Blood Pressure Control in Patients With Mild to Moderate Hypertension in Sri Lanka: A Randomized Clinical Trial
- PMID: 30120478
- PMCID: PMC6583010
- DOI: 10.1001/jama.2018.10359
Fixed Low-Dose Triple Combination Antihypertensive Medication vs Usual Care for Blood Pressure Control in Patients With Mild to Moderate Hypertension in Sri Lanka: A Randomized Clinical Trial
Erratum in
-
Minor Errors to Power Calculation Information.JAMA. 2018 Nov 13;320(18):1940. doi: 10.1001/jama.2018.17363. JAMA. 2018. PMID: 30422180 Free PMC article. No abstract available.
Abstract
Importance: Poorly controlled hypertension is a leading global public health problem requiring new treatment strategies.
Objective: To assess whether a low-dose triple combination antihypertensive medication would achieve better blood pressure (BP) control vs usual care.
Design, setting, and participants: Randomized, open-label trial of a low-dose triple BP therapy vs usual care for adults with hypertension (systolic BP >140 mm Hg and/or diastolic BP >90 mm Hg; or in patients with diabetes or chronic kidney disease: >130 mm Hg and/or >80 mm Hg) requiring initiation (untreated patients) or escalation (patients receiving monotherapy) of antihypertensive therapy. Patients were enrolled from 11 urban hospital clinics in Sri Lanka from February 2016 to May 2017; follow-up ended in October 2017.
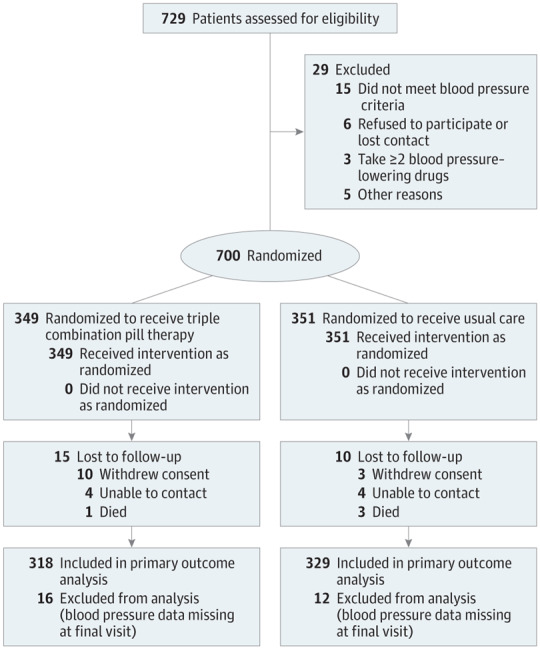
Interventions: A once-daily fixed-dose triple combination pill (20 mg of telmisartan, 2.5 mg of amlodipine, and 12.5 mg of chlorthalidone) therapy (n = 349) or usual care (n = 351).
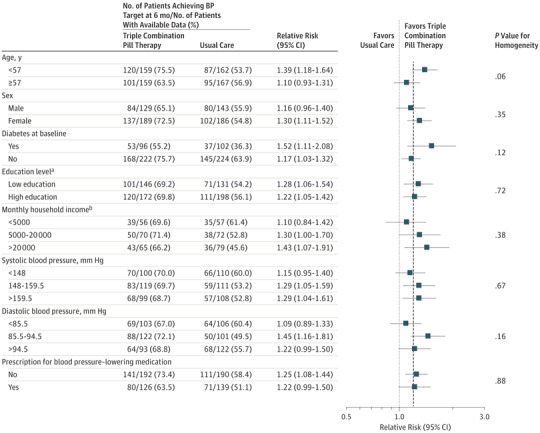
Main outcomes and measures: The primary outcome was the proportion achieving target systolic/diastolic BP (<140/90 mm Hg or <130/80 mm Hg in patients with diabetes or chronic kidney disease) at 6 months. Secondary outcomes included mean systolic/diastolic BP difference during follow-up and withdrawal of BP medications due to an adverse event.
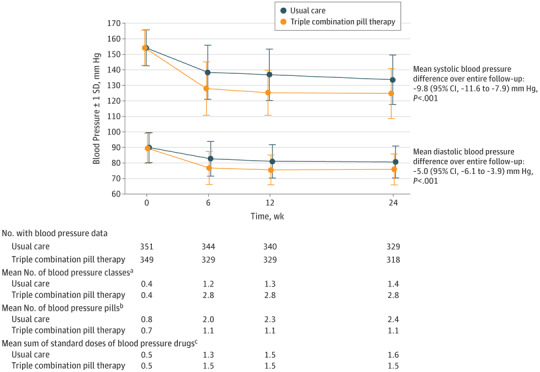
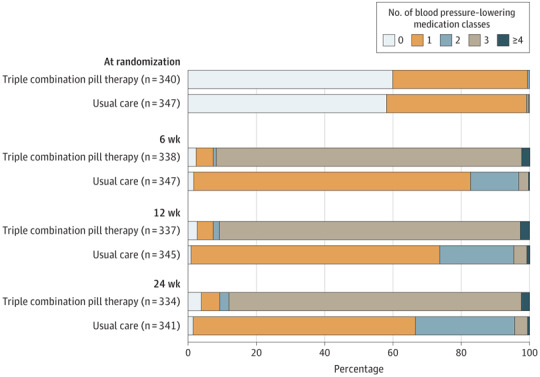
Results: Among 700 randomized patients (mean age, 56 years; 58% women; 29% had diabetes; mean baseline systolic/diastolic BP, 154/90 mm Hg), 675 (96%) completed the trial. The triple combination pill increased the proportion achieving target BP vs usual care at 6 months (70% vs 55%, respectively; risk difference, 12.7% [95% CI, 3.2% to 22.0%]; P < .001). Mean systolic/diastolic BP at 6 months was 125/76 mm Hg for the triple combination pill vs 134/81 mm Hg for usual care (adjusted difference in postrandomization BP over the entire follow-up: systolic BP, -9.8 [95% CI, -7.9 to -11.6] mm Hg; diastolic BP, -5.0 [95% CI, -3.9 to -6.1] mm Hg; P < .001 for both comparisons). Overall, 419 adverse events were reported in 255 patients (38.1% for triple combination pill vs 34.8% for usual care) with the most common being musculoskeletal pain (6.0% and 8.0%, respectively) and dizziness, presyncope, or syncope (5.2% and 2.8%). There were no significant between-group differences in the proportion of patient withdrawal from BP-lowering therapy due to adverse events (6.6% for triple combination pill vs 6.8% for usual care).
Conclusions and relevance: Among patients with mild to moderate hypertension, treatment with a pill containing low doses of 3 antihypertensive drugs led to an increased proportion of patients achieving their target BP goal vs usual care. Use of such medication as initial therapy or to replace monotherapy may be an effective way to improve BP control.
Trial registration: anzctr.org.au Identifier: ACTRN12612001120864; slctr.lk Identifier: SLCTR/2015/020.
Conflict of interest statement
Figures
Comment in
-
Low-Dose Combination Blood Pressure Pharmacotherapy to Improve Treatment Effectiveness, Safety, and Efficiency.JAMA. 2018 Aug 14;320(6):552-554. doi: 10.1001/jama.2018.10649. JAMA. 2018. PMID: 30120460 No abstract available.
-
In persistent hypertension, low-dose triple-pill therapy increased the likelihood of achieving target BP at 6 mo.Ann Intern Med. 2018 Nov 20;169(10):JC56. doi: 10.7326/ACPJC-2018-169-10-056. Ann Intern Med. 2018. PMID: 30452563 No abstract available.
References
-
- Khatib R, McKee M, Shannon H, et al. . Availability and affordability of cardiovascular disease medicines and their effect on use in high-income, middle-income, and low-income countries. Lancet. 2016;387(10013):61-69. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
