

Comparison of central laboratory assessments of ER, PR, HER2, and Ki67 by IHC/FISH and the corresponding mRNAs (ESR1, PGR, ERBB2, and MKi67) by RT-qPCR on an automated, broadly deployed diagnostic platform
- PMID: 30120700
- PMCID: PMC6208911
- DOI: 10.1007/s10549-018-4889-5
Comparison of central laboratory assessments of ER, PR, HER2, and Ki67 by IHC/FISH and the corresponding mRNAs (ESR1, PGR, ERBB2, and MKi67) by RT-qPCR on an automated, broadly deployed diagnostic platform
Abstract
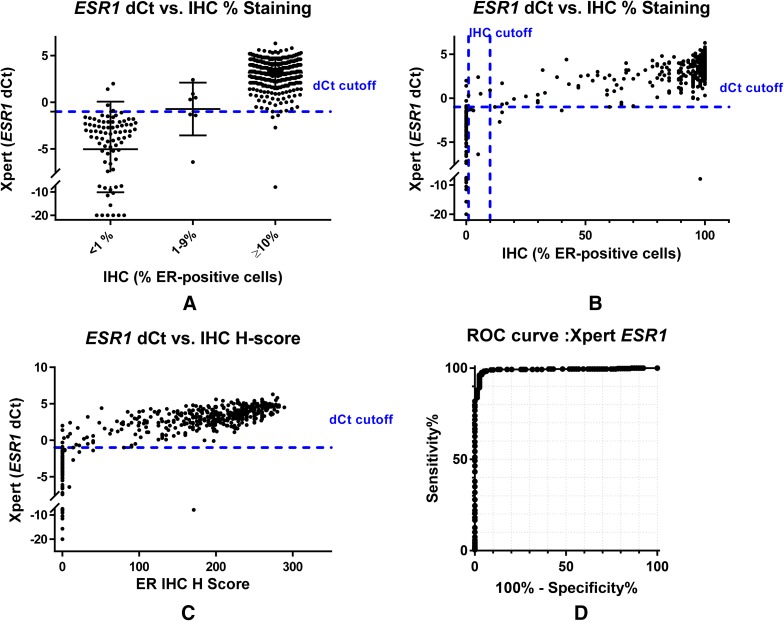
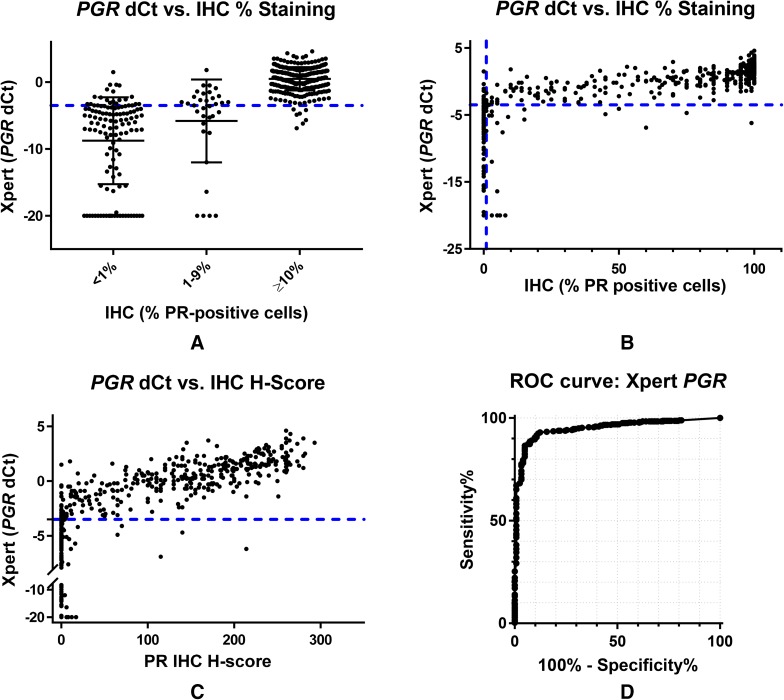
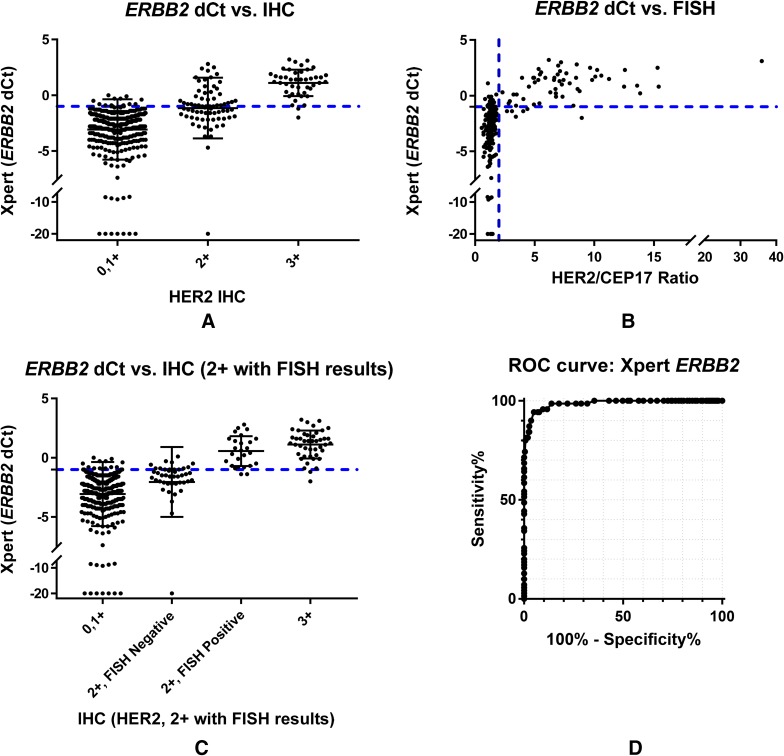
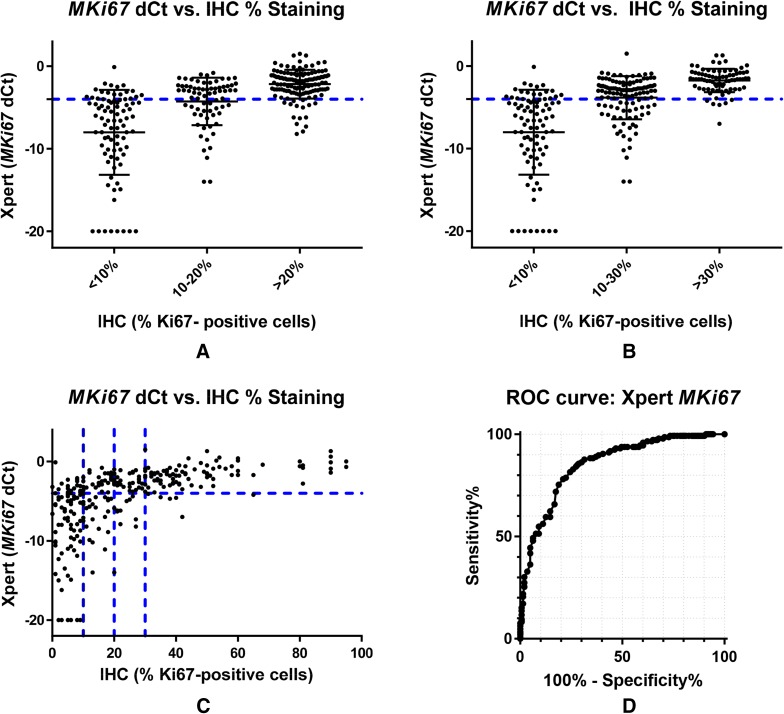
Purpose: The methods (IHC/FISH) typically used to assess ER, PR, HER2, and Ki67 in FFPE specimens from breast cancer patients are difficult to set up, perform, and standardize for use in low and middle-income countries. Use of an automated diagnostic platform (GeneXpert®) and assay (Xpert® Breast Cancer STRAT4) that employs RT-qPCR to quantitate ESR1, PGR, ERBB2, and MKi67 mRNAs from formalin-fixed, paraffin-embedded (FFPE) tissues facilitates analyses in less than 3 h. This study compares breast cancer biomarker analyses using an RT-qPCR-based platform with analyses using standard IHC and FISH for assessment of the same biomarkers.
Methods: FFPE tissue sections from 523 patients were sent to a College of American Pathologists-certified central reference laboratory to evaluate concordance between IHC/FISH and STRAT4 using the laboratory's standard of care methods. A subset of 155 FFPE specimens was tested for concordance with STRAT4 using different IHC antibodies and scoring methods.
Results: Concordance between STRAT4 and IHC was 97.8% for ESR1, 90.4% for PGR, 93.3% for ERBB2 (IHC/FISH for HER2), and 78.6% for MKi67. Receiver operating characteristic curve (ROC) area under the curve (AUC) values of 0.99, 0.95, 0.99, and 0.85 were generated for ESR1, PGR, ERBB2, and MKi67, respectively. Minor variabilities were observed depending on the IHC antibody comparator used.
Conclusion: Evaluation of breast cancer biomarker status by STRAT4 was highly concordant with central IHC/FISH in this blinded, retrospectively analyzed collection of samples. STRAT4 may provide a means to cost-effectively generate standardized diagnostic results for breast cancer patients in low- and middle-income countries.
Keywords: Breast cancer biomarker assays; Estrogen receptor; FISH; Human epidermal growth factor receptor 2; IHC; Progesterone receptor; STRAT4; Tumor proliferation rate.
Conflict of interest statement
Conflict of interest
Authors NCW, WW, KEH, VCC, and AR declared themselves to be employees of Cepheid and have received remuneration from Cepheid. Author SD declared no conflict of interest. Author DK declared no conflict of interest. Author RM declared no conflict of interest. Author JJ declared being a consultant for Bristol-Myers-Squib and G1 Therapeutics. Author RD declared no conflict of interest. Author WB declared no conflict of interest. Author BR declared no conflict of interest. Author TF declared no conflict of interest. Author JLK and MS are employees of Molecular Pathology Laboratory Network, Inc. and declared receiving remuneration from Molecular Pathology Laboratory Network, Inc. Author SC declared no conflict of interest. Author HJ declared remuneration and stock ownership from Indivumed. Authors JMW and MB declared receiving remuneration from Cepheid and stock ownership from Danaher. Author MFP declared consulting for Brogent International LLC and his institution has received research grants for his laboratory from Cepheid, Eli Lilly and Company, Novartis Pharmaceuticals Corporation, Pfizer Inc, F. Hoffmann-La Roche Ltd, and Zymeworks.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the respective institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. This article does not contain any studies with animals performed by any of the authors.
Informed consent
Informed consent was obtained from individual participants included in the study by Indivumed.
Figures
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
