

Predictors of insufficient peak amikacin concentration in critically ill patients on extracorporeal membrane oxygenation
- PMID: 30121083
- PMCID: PMC6098833
- DOI: 10.1186/s13054-018-2122-x
Predictors of insufficient peak amikacin concentration in critically ill patients on extracorporeal membrane oxygenation
Abstract
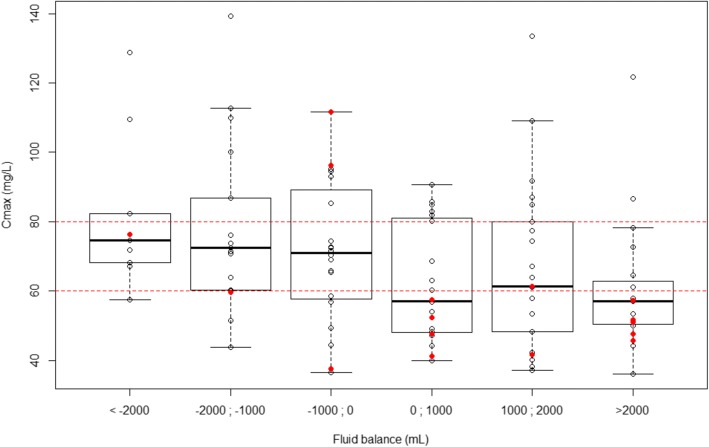
Background: Amikacin infusion requires targeting a peak serum concentration (Cmax) 8-10 times the minimal inhibitory concentration, corresponding to a Cmax of 60-80 mg/L for the least susceptible bacteria to theoretically prevent therapeutic failure. Because drug pharmacokinetics on extracorporeal membrane oxygenation (ECMO) are challenging, we undertook this study to assess the frequency of insufficient amikacin Cmax in critically ill patients on ECMO and to identify relative risk factors.
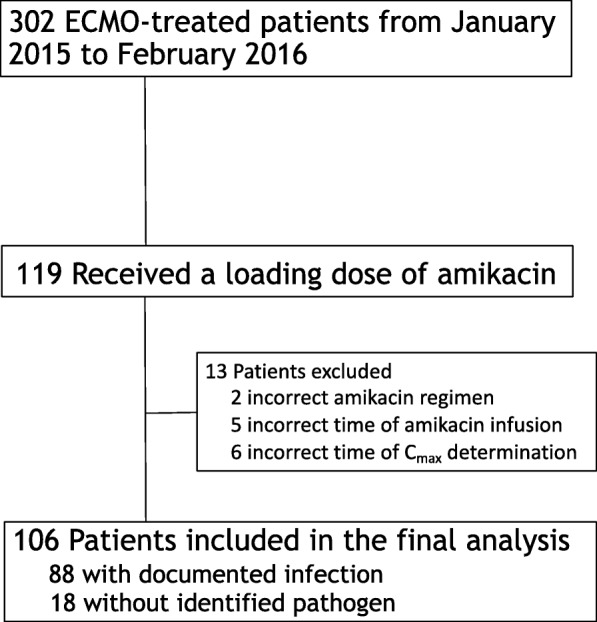
Methods: This was a prospective, observational, monocentric study in a university hospital. Patients on ECMO who received an amikacin loading dose for suspected Gram-negative infections were included. The amikacin loading dose of 25 mg/kg total body weight was administered intravenously and Cmax was measured 30 min after the end of the infusion. Independent predicators of Cmax < 60 mg/L after the first amikacin infusion were identified with mixed-model multivariable analyses. Various dosing simulations were performed to assess the probability of reaching 60 mg/L < Cmax < 80 mg/L.
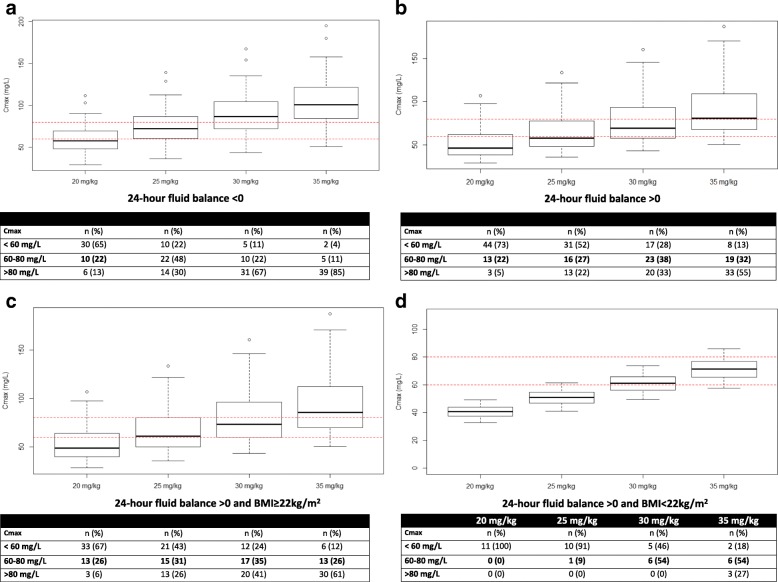
Results: A total of 106 patients on venoarterial ECMO (VA-ECMO) (68%) or venovenous-ECMO (32%) were included. At inclusion, their median (1st; 3rd quartile) Sequential Organ-Failure Assessment score was 15 (12; 18) and 54 patients (51%) were on renal replacement therapy. Overall ICU mortality was 54%. Cmax was < 60 mg/L in 41 patients (39%). Independent risk factors for amikacin under-dosing were body mass index (BMI) < 22 kg/m2 and a positive 24-h fluid balance. Using dosing simulation, increasing the amikacin dosing regimen to 30 mg/kg and 35 mg/kg of body weight when the 24-h fluid balance is positive and the BMI is ≥ 22 kg/m2 or < 22 kg/m2 (Table 3), respectively, would have potentially led to the therapeutic target being reached in 42% of patients while reducing under-dosing to 23% of patients.
Conclusions: ECMO-treated patients were under-dosed for amikacin in one third of cases. Increasing the dose to 35 mg/kg of body weight in low-BMI patients and those with positive 24-h fluid balance on ECMO to reach adequate targeted concentrations should be investigated.
Keywords: Acute respiratory distress syndrome; Amikacin; Cardiac failure; Pharmacokinetics; Shock; Volume of distribution.
Conflict of interest statement
Ethics approval and consent to participate
The study protocol was in accordance with the ethical standards of our hospital’s Institutional Review Board (Committee for the Protection of Human Subjects). In accordance with French law, informed consent was not obtained for demographic, physiological and hospital-outcome data analyses because this observational study did not modify existing diagnostic or therapeutic strategies. However, patients and/or relatives were informed about the anonymous data collection and that they could decline inclusion. This database was registered at the Commission Nationale l’Informatique et des Libertés (CNIL, registration number 1950673).
Consent for publication
In accordance with French law, informed consent was not obtained for demographic, physiological and hospital-outcome data analyses because this observational study did not modify existing diagnostic or therapeutic strategies. However, patients and/or relatives were informed about the anonymous data collection and that they could decline inclusion.
Competing interests
Alain Combes has received lecture fees from Baxter and Gettinge and is the primary investigator of the EOLIA trial (NCT01470703), partly supported by Maquet-Gettinge. Matthieu Schmidt has received lectures fees from Gettinge and Dräger. The remaining authors have no conflicts of interest.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
Similar articles
-
Predictors of insufficient amikacin peak concentration in critically ill patients receiving a 25 mg/kg total body weight regimen.Intensive Care Med. 2014 Jul;40(7):998-1005. doi: 10.1007/s00134-014-3276-x. Epub 2014 Apr 1. Intensive Care Med. 2014. PMID: 24687298
-
Population pharmacokinetics of intravenous sufentanil in critically ill patients supported with extracorporeal membrane oxygenation therapy.Crit Care. 2019 Jul 9;23(1):248. doi: 10.1186/s13054-019-2508-4. Crit Care. 2019. PMID: 31288863 Free PMC article.
-
Early vancomycin, amikacin and gentamicin concentrations in pulmonary artery and pulmonary tissue are not affected by VA ECMO (venoarterial extracorporeal membrane oxygenation) in a pig model of prolonged cardiac arrest.Pulm Pharmacol Ther. 2013 Dec;26(6):655-60. doi: 10.1016/j.pupt.2013.03.008. Epub 2013 Mar 21. Pulm Pharmacol Ther. 2013. PMID: 23524014
-
Extracorporeal membrane oxygenation in the treatment of poisoned patients.Clin Toxicol (Phila). 2013 Jun;51(5):385-93. doi: 10.3109/15563650.2013.800876. Epub 2013 May 23. Clin Toxicol (Phila). 2013. PMID: 23697460 Review.
-
Pharmacokinetic changes of antibiotic, antiviral, antituberculosis and antifungal agents during extracorporeal membrane oxygenation in critically ill adult patients.J Clin Pharm Ther. 2017 Dec;42(6):661-671. doi: 10.1111/jcpt.12636. Epub 2017 Sep 25. J Clin Pharm Ther. 2017. PMID: 28948652 Review.
Cited by
-
Population Pharmacokinetics of Amikacin in Patients on Veno-Arterial Extracorporeal Membrane Oxygenation.Pharmaceutics. 2022 Jan 26;14(2):289. doi: 10.3390/pharmaceutics14020289. Pharmaceutics. 2022. PMID: 35214022 Free PMC article.
-
[Clinical pharmacokinetics of anti-infective drugs in extracorporeal membrane oxygenation].Anaesthesist. 2019 Dec;68(12):821-826. doi: 10.1007/s00101-019-00702-8. Anaesthesist. 2019. PMID: 31740986 Review. German.
-
Ventilator-associated pneumonia in extracorporeal membrane oxygenation-assisted patients.Ann Transl Med. 2018 Nov;6(21):427. doi: 10.21037/atm.2018.10.18. Ann Transl Med. 2018. PMID: 30581835 Free PMC article. Review.
-
Machines that help machines to help patients: optimising antimicrobial dosing in patients receiving extracorporeal membrane oxygenation and renal replacement therapy using dosing software.Intensive Care Med. 2022 Oct;48(10):1338-1351. doi: 10.1007/s00134-022-06847-2. Epub 2022 Aug 23. Intensive Care Med. 2022. PMID: 35997793 Free PMC article. Review.
-
Systematic review of high-dose amikacin regimens for the treatment of Gram-negative infections based on EUCAST dosing recommendations.Eur J Hosp Pharm. 2023 Jul;30(4):189-195. doi: 10.1136/ejhpharm-2022-003421. Epub 2022 Nov 7. Eur J Hosp Pharm. 2023. PMID: 36344247 Free PMC article.
References
-
- Belohlavek J, Springer D, Mlcek M, Huptych M, Boucek T, Hodkova G, et al. Early vancomycin, amikacin and gentamicin concentrations in pulmonary artery and pulmonary tissue are not affected by VA ECMO (venoarterial extracorporeal membrane oxygenation) in a pig model of prolonged cardiac arrest. Pulm Pharmacol Ther. 2013;26:655–660. doi: 10.1016/j.pupt.2013.03.008. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
