

Lower limb perfusion during robotic-assisted laparoscopic radical prostatectomy evaluated by near-infrared spectroscopy: an observational prospective study
- PMID: 30121089
- PMCID: PMC6098825
- DOI: 10.1186/s12871-018-0567-8
Lower limb perfusion during robotic-assisted laparoscopic radical prostatectomy evaluated by near-infrared spectroscopy: an observational prospective study
Abstract
Background: Decreased perfusion in the lower extremities is one of the several adverse effects of placing patients in a lithotomy or Trendelenburg position during surgery. This study aimed to evaluate the effects of patient positioning in lower limb perfusion patients undergoing robotic-assisted laparoscopic radical prostatectomy (RARP) using near-infrared spectroscopy (NIRS).
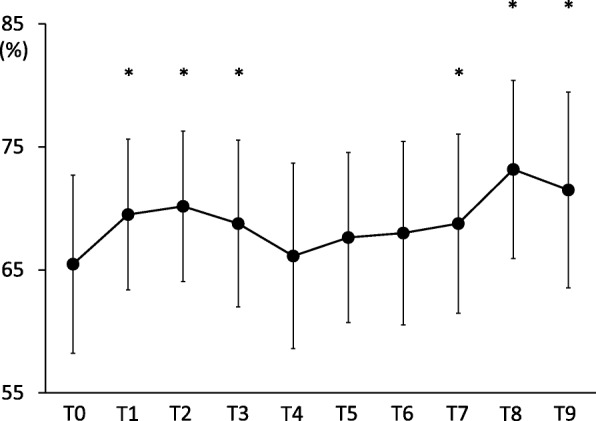
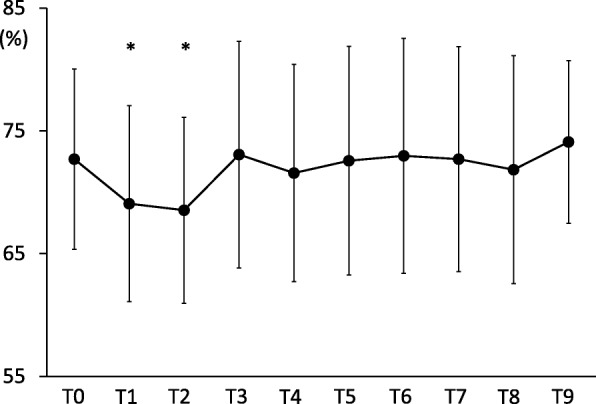
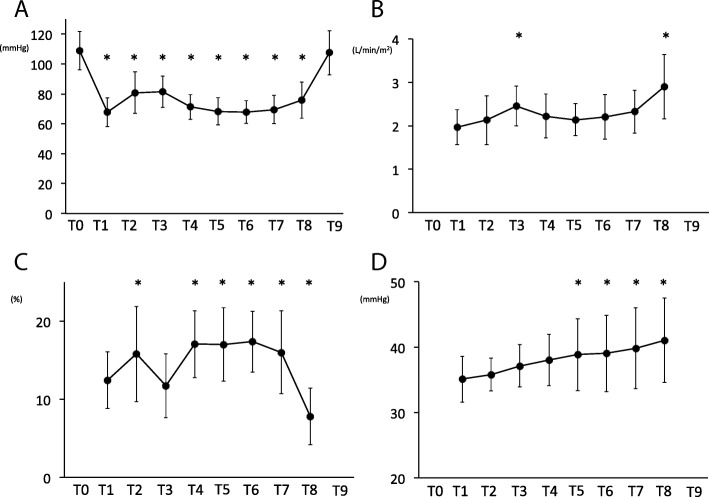
Methods: This observation study comprised 30 consenting males with American Society of Anaesthesiologists physical status classes I and II (age range, ≥20 to < 80 years). Regional saturation of oxygen measurements was obtained using an INVOS™ oximeter (Somanetics, Troy, MI, USA). A NIRS sensor was positioned on the surface of the skin at the mid-diaphyseal region of the calf muscles (the gastrocnemius and soleus), over the posterior compartment, in the right lower leg. Regional saturation of oxygen (rSO2) was sampled during the following time points: before and 5 min after induction of anaesthesia (T0,T1); 5 min after establishment of pneumoperitoneum in a 0° lithotomy position (T2); 5 min after a 25° Trendelenburg position (T3); 30, 60, 90 and 120 min after pneumoperitoneum in a Trendelenburg position (T4, T5, T6 and T7, respectively); after desufflation in a supine position (T8); and after tracheal extubation (T9).
Results: Lower limb perfusion evaluated by NIRS was increased after induction of anaesthesia and maintained during steep Trendelenburg positions in RARP patients with no risk for lower limb compartment syndrome (LLCS) (T0:65 ± 7.2%, T1:69 ± 6.1%, T2:70±:6.1%, T3:68 ± 6.7%, T4:66 ± 7.5%, T5:67 ± 6.9%, T6:68 ± 7.2%, T8:73 ± 7.2%, T9:71 ± 7.9%, respectively).
Conclusions: Lower limb perfusion evaluated by NIRS was maintained during the RARP procedure. Correct patient positioning and careful assessment of risk factors such as vascular morbidity could be important for the prevention of LLCS during RARP.
Keywords: Lithotomy position; Lower limb perfusion; Robotic prostatectomy.
Conflict of interest statement
Ethics approval and consent to participate
This study was approved by the local institutional review board of the Ehime University Graduate School of Medicine (registration number 1308010). After a detailed explanation written informed consent was obtained from 30 patients scheduled for RARP.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
Similar articles
-
Effect of dexmedetomidine on intraocular pressure in patients undergoing robot-assisted laparoscopic radical prostatectomy under total intravenous anesthesia: A randomized, double blinded placebo controlled clinical trial.J Clin Anesth. 2018 Sep;49:30-35. doi: 10.1016/j.jclinane.2018.06.006. Epub 2018 Jun 5. J Clin Anesth. 2018. PMID: 29883964 Clinical Trial.
-
The effects of different positions on lower extremity hemodynamics during robot-assisted laparoscopic radical prostatectomy for prostate cancer.BMC Urol. 2024 Apr 20;24(1):92. doi: 10.1186/s12894-024-01462-3. BMC Urol. 2024. PMID: 38643097 Free PMC article.
-
The effect of pneumoperitoneum in the steep Trendelenburg position on cerebral oxygenation.Acta Anaesthesiol Scand. 2009 Aug;53(7):895-9. doi: 10.1111/j.1399-6576.2009.01991.x. Epub 2009 May 6. Acta Anaesthesiol Scand. 2009. PMID: 19426238
-
Intraoperative peripheral nerve injury related to lithotomy positioning with steep Trendelenburg in patients undergoing robotic-assisted laparoscopic surgery - A systematic review.J Adv Nurs. 2020 Feb;76(2):490-503. doi: 10.1111/jan.14271. Epub 2019 Dec 2. J Adv Nurs. 2020. PMID: 31736124
-
Anesthetic concerns for robotic-assisted laparoscopic radical prostatectomy.Minerva Anestesiol. 2012 May;78(5):596-604. Epub 2012 Mar 13. Minerva Anestesiol. 2012. PMID: 22415437 Review.
Cited by
-
Hypoxemia of the lower limbs during robot-assisted radical prostatectomy in Trendelenburg position.BJUI Compass. 2023 Oct 9;5(2):313-318. doi: 10.1002/bco2.296. eCollection 2024 Mar. BJUI Compass. 2023. PMID: 38371210 Free PMC article.
-
Positioning patients for robotic-assisted surgery: A qualitative study of operating room nurses' experiences.Nurs Open. 2023 Feb;10(2):469-478. doi: 10.1002/nop2.1312. Epub 2022 Aug 12. Nurs Open. 2023. PMID: 36631733 Free PMC article.
-
Anesthesia for robot-assisted surgery: a review.Anaesthesiol Intensive Ther. 2025 May 26;57(1):99-107. doi: 10.5114/ait/203168. Anaesthesiol Intensive Ther. 2025. PMID: 40420612 Free PMC article. Review.
-
Well-Leg Compartment Syndrome After Percutaneous Nephrolithotomy in the Galdakao-Modified Supine Valdivia Position.Res Rep Urol. 2020 Jul 24;12:295-302. doi: 10.2147/RRU.S259357. eCollection 2020. Res Rep Urol. 2020. PMID: 32802806 Free PMC article.
-
Effect of intraoperative operating table rotation on lower limb perfusion index in patients in the lithotomy position.Medicine (Baltimore). 2022 Sep 23;101(38):e30412. doi: 10.1097/MD.0000000000030677. Medicine (Baltimore). 2022. PMID: 36197219 Free PMC article.
References
-
- Meyer RS, White KK, Smith JM, Groppo ER, Mubarak SJ, Hargens AR. Intramuscular and blood pressures in legs positioned in the hemilithotomy position: clarification of risk factors for well-leg acute compartment syndrome. J Bone Joint Surg Am. 2002;84:1829–1835. doi: 10.2106/00004623-200210000-00014. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
