

Brentuximab vedotin with gemcitabine for paediatric and young adult patients with relapsed or refractory Hodgkin's lymphoma (AHOD1221): a Children's Oncology Group, multicentre single-arm, phase 1-2 trial
- PMID: 30122620
- PMCID: PMC6487196
- DOI: 10.1016/S1470-2045(18)30426-1
Brentuximab vedotin with gemcitabine for paediatric and young adult patients with relapsed or refractory Hodgkin's lymphoma (AHOD1221): a Children's Oncology Group, multicentre single-arm, phase 1-2 trial
Abstract
Background: Patients with primary refractory Hodgkin's lymphoma or early relapse have a poor prognosis. Although many salvage regimens have been developed, there is no standard of care. Brentuximab vedotin and gemcitabine have been shown to be active in patients with relapsed or refractory Hodgkin's lymphoma when used as monotherapy, and each has been successfully used in combination with other agents. Preclinical data suggest that brentuximab vedotin can sensitise lymphoma cells to gemcitabine, supporting the use of the combination. We aimed to define the safety and efficacy of brentuximab vedotin with gemcitabine in children and young adults with primary refractory Hodgkin's lymphoma or early relapse.
Methods: In this Children's Oncology Group, multicentre, single-arm, phase 1-2 trial, we recruited patients with Hodgkin's lymphoma from hospitals across the USA and Canada. Eligible patients were aged younger than 30 years, had no previous brentuximab vedotin exposure, and had primary refractory disease or relapse of less than 1 year from completion of initial treatment. Each 21-day cycle consisted of 1000 mg/m2 intravenous gemcitabine on days 1 and 8 and intravenous brentuximab vedotin on day 1 at 1·4 mg/kg or 1·8 mg/kg. The primary objectives were to establish the recommended phase 2 dose of brentuximab vedotin in this combination, the safety of the combination, and the proportion of patients who achieved a complete response among those treated at the recommended phase 2 level, within four cycles of treatment. This trial is registered with ClinicalTrials.gov, number NCT01780662.
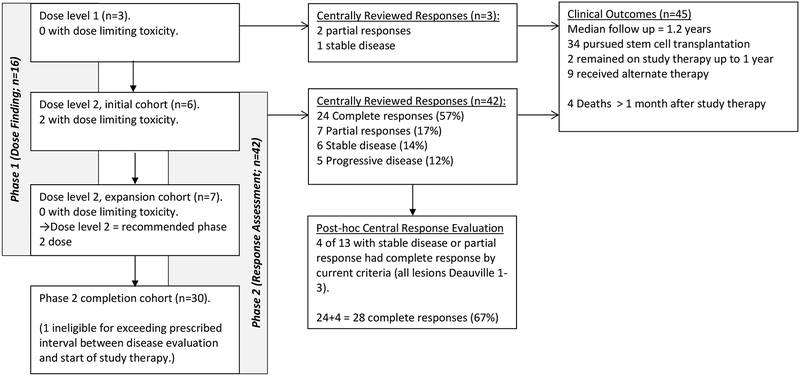
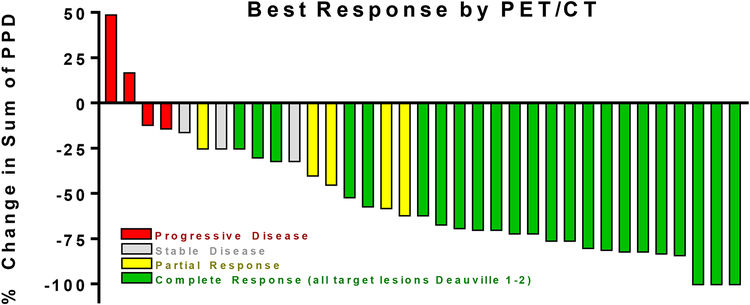
Findings: Between Feb 5, 2013, and Aug 19, 2016, 46 patients were enrolled, including one who was found to be ineligible, in the two phases of the study. The recommended phase 2 dose of brentuximab vedotin was 1·8 mg/kg in combination with gemcitabine 1000 mg/m2. 24 (57%) of 42 evaluable patients (95% CI 41-72) given this dose level had a complete response within the first four cycles of treatment. Four (31%) of 13 patients with a partial response or stable disease had all target lesions with Deauville scores of 3 or less after cycle 4. By modern response criteria, these were also complete responses (total number with complete response 28 [67%] of 42 [95% CI 51-80]). The most common grade 3-4 adverse events in all 42 participants treated at the recommended phase 2 dose were neutropenia (15 [36%]), rash (15 [36%]), transaminitis (9 [21%]), and pruritus (4 [10%]). There were no treatment-related deaths.
Interpretation: Brentuximab vedotin with gemcitabine is a safe combination treatment with a tolerable toxicity profile for patients with primary refractory Hodgkin's lymphoma or high-risk relapse. The preliminary activity of this combination shown in this trial warrants further investigation in randomised controlled trials.
Funding: National Institutes of Health and the St. Baldrick's Foundation.
Copyright © 2018 Elsevier Ltd. All rights reserved.
Figures
Comment in
-
Brentuximab vedotin-based salvage treatment in Hodgkin's lymphoma.Lancet Oncol. 2018 Sep;19(9):1144-1146. doi: 10.1016/S1470-2045(18)30510-2. Epub 2018 Aug 16. Lancet Oncol. 2018. PMID: 30122617 No abstract available.
References
-
- Kelly KM. Hodgkin lymphoma in children and adolescents: improving the therapeutic index. Blood. 2015;126(22):2452–8. - PubMed
-
- Harker-Murray PD, Drachtman RA, Hodgson DC, Chauvenet AR, Kelly KM, Cole PD. Stratification of treatment intensity in relapsed pediatric Hodgkin lymphoma. Pediatric Blood & Cancer. 2014;61(4):579–86. - PubMed
-
- Michallet A-S, Guillermin Y, Deau B, Lebras L, Harel S, Amorin S, et al. Sequential combination of gemcitabine, vinorelbine, pegylated liposomal doxorubicin and brentuximab as a bridge regimen to transplant in relapsed or refractory Hodgkin lymphoma. Haematologica. 2015;100(7):e269–e71. - PMC - PubMed
-
- Younes A, Connors JM, Park SI, Fanale M, O’Meara MM, Hunder NN, et al. Brentuximab vedotin combined with ABVD or AVD for patients with newly diagnosed Hodgkin’s lymphoma: a phase 1, open-label, dose-escalation study. The Lancet Oncology. 2013;14(13):1348–56. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
