

2017 WSES guidelines on colon and rectal cancer emergencies: obstruction and perforation
- PMID: 30123315
- PMCID: PMC6090779
- DOI: 10.1186/s13017-018-0192-3
2017 WSES guidelines on colon and rectal cancer emergencies: obstruction and perforation
Abstract
ᅟ: Obstruction and perforation due to colorectal cancer represent challenging matters in terms of diagnosis, life-saving strategies, obstruction resolution and oncologic challenge. The aims of the current paper are to update the previous WSES guidelines for the management of large bowel perforation and obstructive left colon carcinoma (OLCC) and to develop new guidelines on obstructive right colon carcinoma (ORCC).
Methods: The literature was extensively queried for focused publication until December 2017. Precise analysis and grading of the literature has been performed by a working group formed by a pool of experts: the statements and literature review were presented, discussed and voted at the Consensus Conference of the 4th Congress of the World Society of Emergency Surgery (WSES) held in Campinas in May 2017.
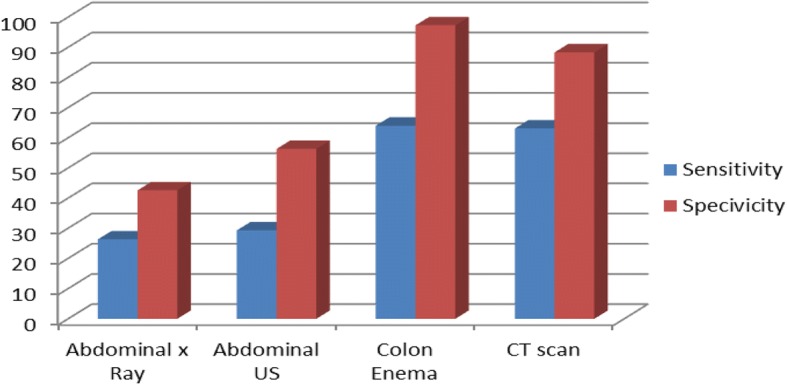
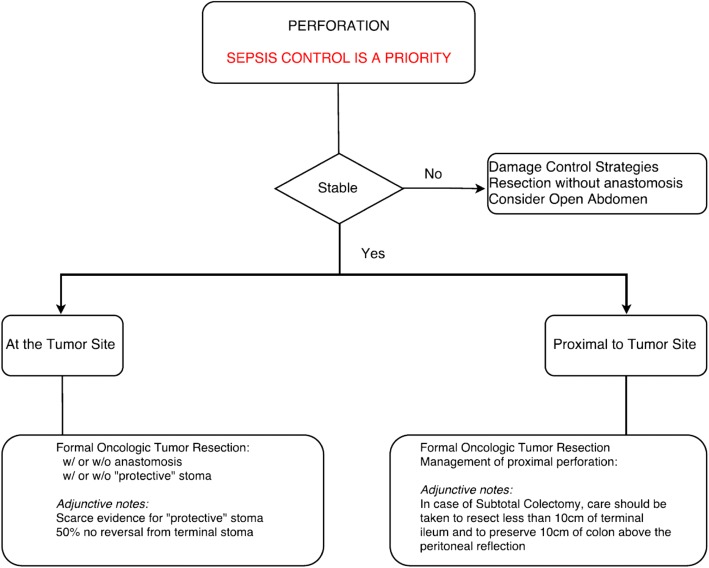
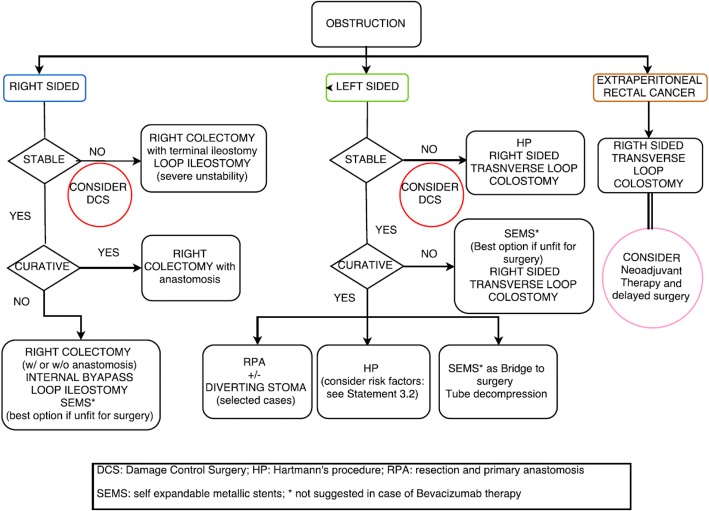
Results: CT scan is the best imaging technique to evaluate large bowel obstruction and perforation. For OLCC, self-expandable metallic stent (SEMS), when available, offers interesting advantages as compared to emergency surgery; however, the positioning of SEMS for surgically treatable causes carries some long-term oncologic disadvantages, which are still under analysis. In the context of emergency surgery, resection and primary anastomosis (RPA) is preferable to Hartmann's procedure, whenever the characteristics of the patient and the surgeon are permissive. Right-sided loop colostomy is preferable in rectal cancer, when preoperative therapies are predicted.With regards to the treatment of ORCC, right colectomy represents the procedure of choice; alternatives, such as internal bypass and loop ileostomy, are of limited value.Clinical scenarios in the case of perforation might be dramatic, especially in case of free faecal peritonitis. The importance of an appropriate balance between life-saving surgical procedures and respect of oncologic caveats must be stressed. In selected cases, a damage control approach may be required.Medical treatments including appropriate fluid resuscitation, early antibiotic treatment and management of co-existing medical conditions according to international guidelines must be delivered to all patients at presentation.
Conclusions: The current guidelines offer an extensive overview of available evidence and a qualitative consensus regarding management of large bowel obstruction and perforation due to colorectal cancer.
Keywords: Cancer; Colon; Emergency; Obstruction; Perforation; Rectum.
Conflict of interest statement
Not applicable. Not applicable. The authors declare that they have no competing interests. Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Ansaloni L, Andersson RE, Bazzoli F, Catena F, Cennamo V, Di Saverio S, Fuccio L, Jeekel H, Leppaniemi A, Moore E, Pinna AD, Pisano M, Repici A, Sugarbaker PH, Tuech JJ. Guidelines in the management of obstructing cancer of the left colon: consensus conference of the world society of emergency surgery (WSES) and peritoneum and surgery (PnS) society. World J Emerg Surg. 2010;5:29. doi: 10.1186/1749-7922-5-29. - DOI - PMC - PubMed
-
- Benson AB, 3rd, Venook AP, Cederquist L, Chan E, Chen YJ, Cooper HS, Deming D, Engstrom PF, Enzinger PC, Fichera A, Grem JL, Grothey A, Hochster HS, Hoffe S, Hunt S, Kamel A, Kirilcuk N, Krishnamurthi S, Messersmith WA, Mulcahy MF, Murphy JD, Nurkin S, Saltz L, Sharma S, Shibata D, Skibber JM, Sofocleous CT, Stoffel EM, Stotsky-Himelfarb E, Willett CG, Wu CS, Gregory KM, Freedman-Cass D. Colon cancer, version 1.2017, NCCN Clinical Practice Guidelines in Oncology. J Natl Compr Canc Netw. 2017;15(3):370–398. doi: 10.6004/jnccn.2017.0036. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
