

Population Pharmacokinetics of the Interleukin-23 Inhibitor Risankizumab in Subjects with Psoriasis and Crohn's Disease: Analyses of Phase I and II Trials
- PMID: 30123942
- PMCID: PMC6373392
- DOI: 10.1007/s40262-018-0704-z
Population Pharmacokinetics of the Interleukin-23 Inhibitor Risankizumab in Subjects with Psoriasis and Crohn's Disease: Analyses of Phase I and II Trials
Abstract
Background and objectives: Risankizumab is a humanized anti-interleukin-23 monoclonal antibody in development for the treatment of several inflammatory diseases. This work characterized the pharmacokinetics of risankizumab and evaluated covariates that may affect its exposures using phase I and II trial data in subjects with psoriasis and Crohn's disease.
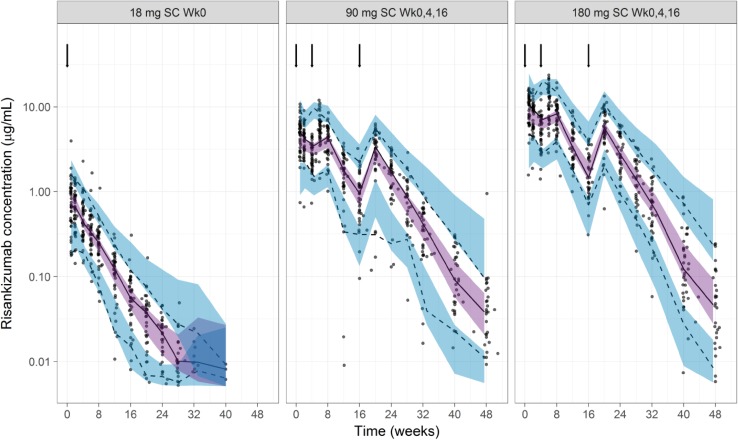
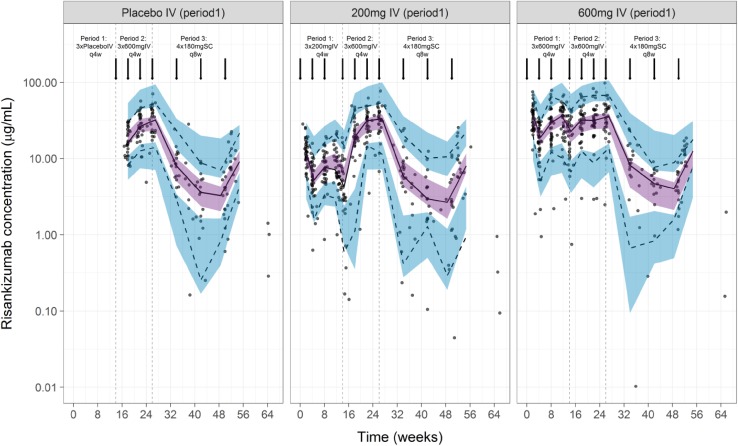
Methods: Plasma concentration measurements from a phase I study and a phase II study in subjects with psoriasis (n = 157; single doses of 0.01-5 mg/kg intravenously, 0.25-1 mg/kg subcutaneously, and 18 mg subcutaneously, and multiple doses of 90 and 180 mg subcutaneously), and a phase II study in subjects with Crohn's disease (n = 115; doses of 200 or 600 mg intravenously every 4 weeks followed by 180 mg subcutaneously every 8 weeks) were analyzed using non-linear mixed-effects modeling. The model was qualified using bootstrap and simulation-based diagnostics.
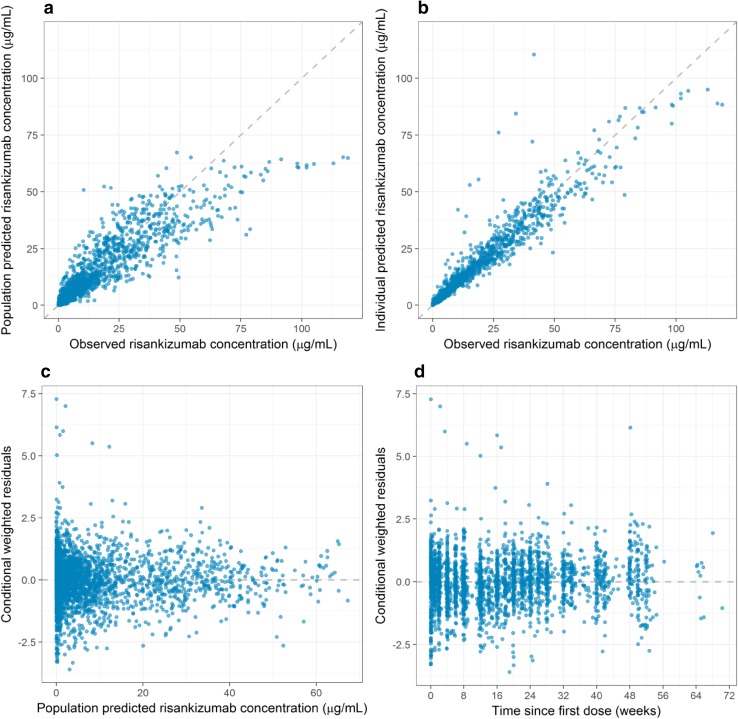
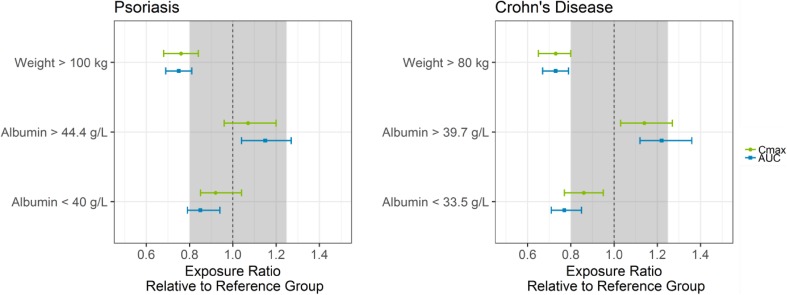
Results: A two-compartment model with first-order absorption and elimination described the pharmacokinetics of risankizumab. Considering the body weight and baseline albumin central tendency differences between disease populations, risankizumab clearance, steady-state volume of distribution, and terminal-phase elimination half-life were estimated to be approximately 0.35 L/day, 11.7 L, and 27 days, respectively, for a typical 90-kg subject with psoriasis with an albumin level of 42 g/L, and 0.31 L/day, 8.45 L, and 22 days, respectively, for a typical 65-kg subject with Crohn's disease with an albumin level of 37 g/L. Risankizumab absolute subcutaneous bioavailability and absorption rate constant were 72% and 0.18 day-1, respectively. Inter-individual variability for clearance was 37%.
Conclusions: Risankizumab displayed pharmacokinetic characteristics typical for an IgG1 monoclonal antibody with no apparent target-mediated disposition. Accounting for the effects of body weight and baseline albumin explained the small differences in the pharmacokinetics of risankizumab between psoriasis and Crohn's disease, with no further differences between the patient populations.
Conflict of interest statement
Conflict of interest
All authors are employees of AbbVie and may hold AbbVie stock or stock options.
Ethics Approval
Studies included in the analyses were conducted in accordance with Good Clinical Practice guidelines and the ethical principles that have their origin in the Declaration of Helsinki. The protocols and informed consent forms were approved by the institutional review boards or ethics committees.
Consent to Participate
Participants provided written informed consent before any study-related procedures were performed.
Figures
References
-
- Bowes J, Barton A. The genetics of psoriatic arthritis: lessons from genome-wide association studies. Discov Med. 2010;10(52):177–183. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
