

Percutaneous suction and irrigation for the treatment of recalcitrant pyogenic spondylodiscitis
- PMID: 30123957
- PMCID: PMC6098991
- DOI: 10.1186/s10195-018-0496-9
Percutaneous suction and irrigation for the treatment of recalcitrant pyogenic spondylodiscitis
Abstract
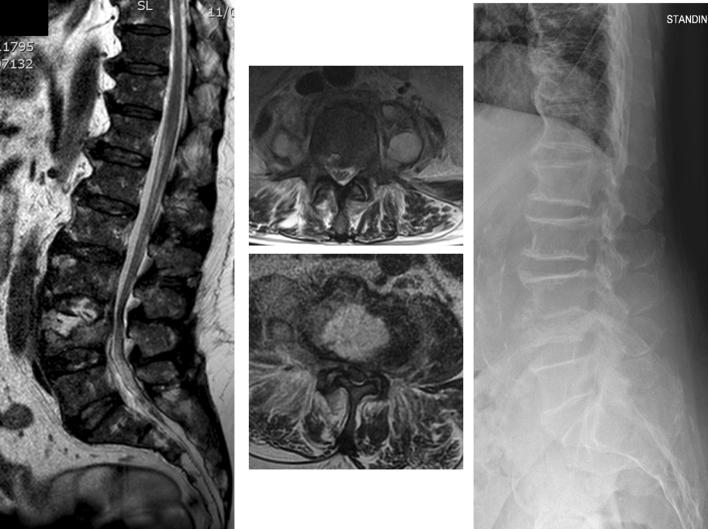
Background: The primary management of pyogenic spondylodiscitis is conservative. Once the causative organism has been identified, by blood culture or biopsy, administration of appropriate intravenous antibiotics is started. Occasionally patients do not respond to antibiotics and surgical irrigation and debridement is needed. The treatment of these cases is challenging and controversial. Furthermore, many affected patients have significant comorbidities often precluding more extensive surgical intervention. The aim of this study is to describe early results of a novel, minimally invasive percutaneous technique for disc irrigation and debridement in pyogenic spondylodiscitis.
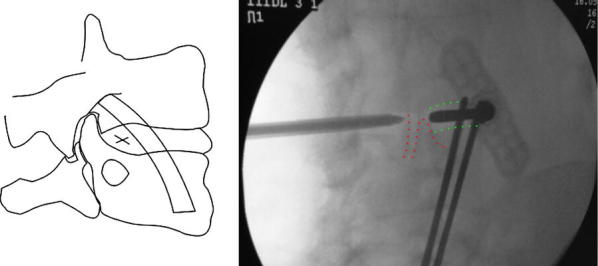
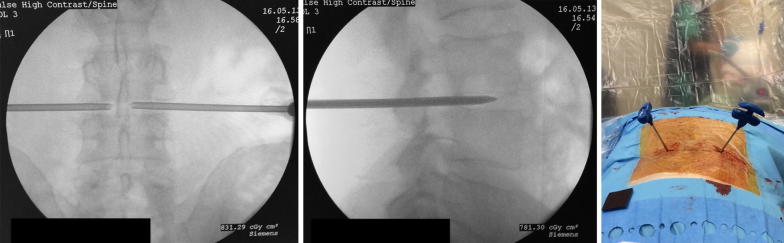
Materials and methods: A series of 10 consecutive patients diagnosed with pyogenic spondylodiscitis received percutaneous disc irrigation and debridement. The procedure was performed by inserting two Jamshidi needles percutaneously into the disc space. Indications for surgery were poor response to antibiotic therapy (8 patients) and the need for more extensive biopsy (2 patients). Pre- and postoperative white blood cell count (WBC), C-reactive protein (CRP), erythrocyte sedimentation rate (ESR), Oswestry disability index (ODI), and visual analogue score (VAS) for back pain were collected. Minimum follow-up was 18 months, with regular interval assessments.
Results: There were 7 males and 3 females with a mean age of 67 years. The mean WBC before surgery was 14.63 × 109/L (10.9-26.4) and dropped to 7.48 × 109/L (5.6-9.8) after surgery. The mean preoperative CRP was 188 mg/L (111-250) and decreased to 13.83 mg/L (5-21) after surgery. Similar improvements were seen with ESR. All patients reported significant improvements in ODI and VAS scores after surgery. The average hospital stay after surgery was 8.17 days. All patients had resolution of the infection, and there were no complications associated with the procedure.
Conclusions: Our study confirms the feasibility and safety of our percutaneous technique for irrigation and debridement of pyogenic spondylodiscitis. Percutaneous irrigation and suction offers a truly minimally invasive option for managing recalcitrant spondylodiscitis or for diagnostic purposes. The approach used is very similar to discography and can be easily adapted to different hospital settings.
Level of evidence: Level III.
Keywords: Minimally invasive technique; Pyogenic spondylodiscitis; Spinal abscess drainage; Spinal percutaneous drainage.
Figures

Similar articles
-
Single-level lumbar pyogenic spondylodiscitis treated with mini-open anterior debridement and fusion in combination with posterior percutaneous fixation via a modified anterior lumbar interbody fusion approach.J Neurosurg Spine. 2015 Dec;23(6):747-53. doi: 10.3171/2015.5.SPINE14876. Epub 2015 Sep 4. J Neurosurg Spine. 2015. PMID: 26340382
-
One-stage Debridement via Oblique Lateral Interbody Fusion Corridor Combined with Posterior Pedicle Screw Fixation in Treating Spontaneous Lumbar Infectious Spondylodiscitis: A Case Series.Orthop Surg. 2019 Dec;11(6):1109-1119. doi: 10.1111/os.12562. Epub 2019 Nov 7. Orthop Surg. 2019. PMID: 31701667 Free PMC article.
-
Continuous Epidural Irrigation and Drainage Combined with Posterior Debridement and Posterior Lumbar Inter-Body Fusion for the Management of Single-Segment Lumbar Pyogenic Spondylodiscitis.Surg Infect (Larchmt). 2020 Apr;21(3):262-267. doi: 10.1089/sur.2019.038. Epub 2019 Oct 24. Surg Infect (Larchmt). 2020. PMID: 31647391
-
Treatment of osteomyelitis of the spine using percutaneous suction/irrigation and percutaneous external spinal fixation.J Spinal Disord. 1994 Jun;7(3):185-205. doi: 10.1097/00002517-199407030-00001. J Spinal Disord. 1994. PMID: 7919642 Review.
-
Minimally Invasive Spine Stabilization for Pyogenic Spondylodiscitis: A 23-Case Series and Review of Literature.Medicina (Kaunas). 2022 Jun 1;58(6):754. doi: 10.3390/medicina58060754. Medicina (Kaunas). 2022. PMID: 35744017 Free PMC article. Review.
Cited by
-
Surgical management of spontaneous thoracic and lumbar spondylodiscitis by fixation and debridement.Surg Neurol Int. 2022 Feb 11;13:44. doi: 10.25259/SNI_1236_2021. eCollection 2022. Surg Neurol Int. 2022. PMID: 35242410 Free PMC article.
-
10-Year Clinical, Functional, and X-ray Follow-Up Evaluation of a Novel Posterior Percutaneous Screw-Rod Instrumentation Technique for Single-Level Pyogenic Spondylodiscitis.Trop Med Infect Dis. 2021 Sep 1;6(3):159. doi: 10.3390/tropicalmed6030159. Trop Med Infect Dis. 2021. PMID: 34564543 Free PMC article.
-
Successful Treatment of Complicated Pyogenic Spondylitis Due to Advanced Rectosigmoid Cancer Utilizing Vigorous Antibiotic Therapy and Minimally Invasive Robotic Colorectal Surgery: A Case Report.Cureus. 2024 Aug 22;16(8):e67536. doi: 10.7759/cureus.67536. eCollection 2024 Aug. Cureus. 2024. PMID: 39310526 Free PMC article.
-
Early surgery with antibiotic medication was effective and efficient in treating pyogenic spondylodiscitis.BMC Musculoskelet Disord. 2021 Mar 18;22(1):288. doi: 10.1186/s12891-021-04155-2. BMC Musculoskelet Disord. 2021. PMID: 33736624 Free PMC article.
-
Percutaneous Endoscopic Interbody Debridement and Fusion (PEIDF) Decreases Risk of Sepsis and Mortality in Treating Infectious Spondylodiscitis for Patients with Poor Physical Status, a Retrospective Cohort Study.Biomedicines. 2022 Jul 10;10(7):1659. doi: 10.3390/biomedicines10071659. Biomedicines. 2022. PMID: 35884964 Free PMC article.
References
-
- Fantoni M, Trecarichi EM, Rossi B, et al. Epidemiological and clinical features of pyogenic spondylodiscitis. Eur Rev Med Pharmacol Sci. 2012;16:2–7. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
