

Pharmacokinetics-Pharmacodynamics of High-Dose Ivermectin with Dihydroartemisinin-Piperaquine on Mosquitocidal Activity and QT-Prolongation (IVERMAL)
- PMID: 30125353
- PMCID: PMC6585895
- DOI: 10.1002/cpt.1219
Pharmacokinetics-Pharmacodynamics of High-Dose Ivermectin with Dihydroartemisinin-Piperaquine on Mosquitocidal Activity and QT-Prolongation (IVERMAL)
Abstract
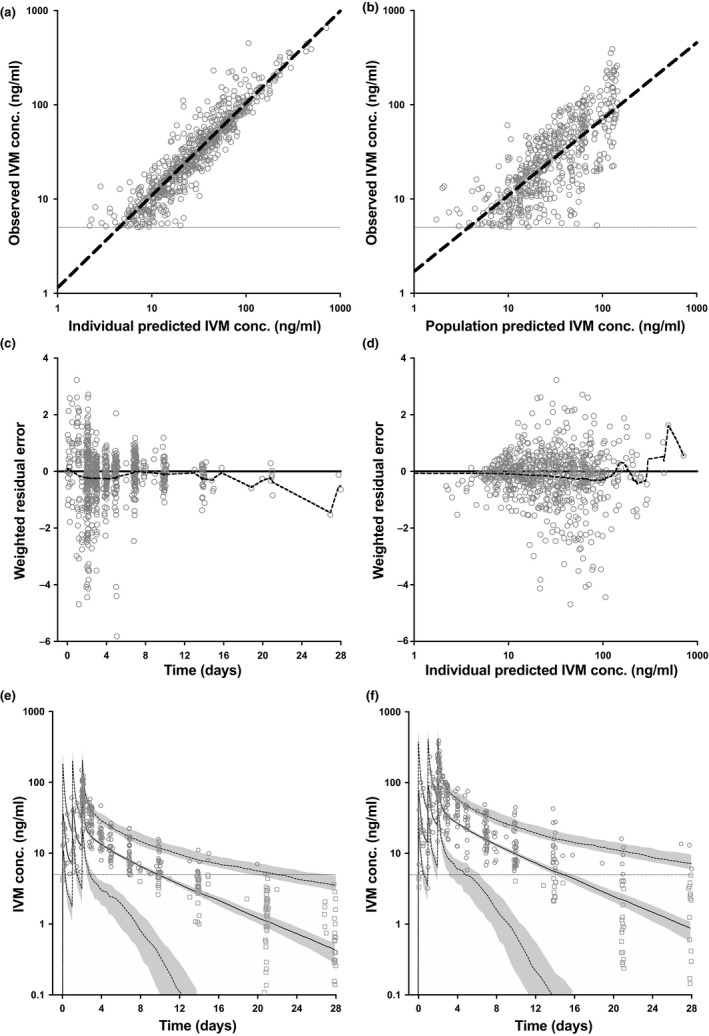
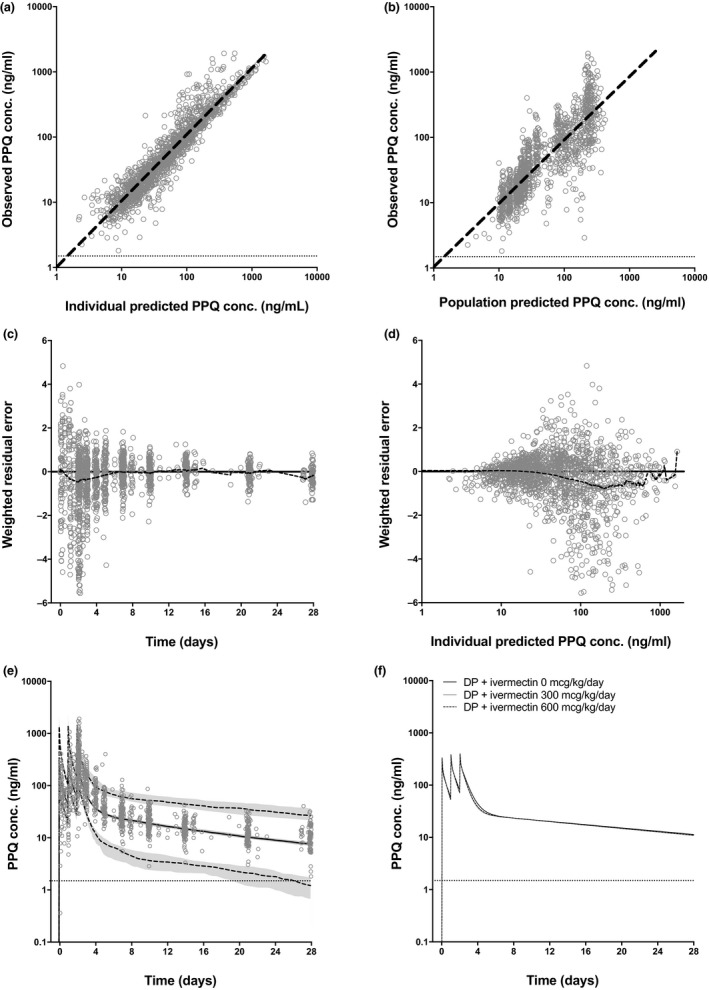
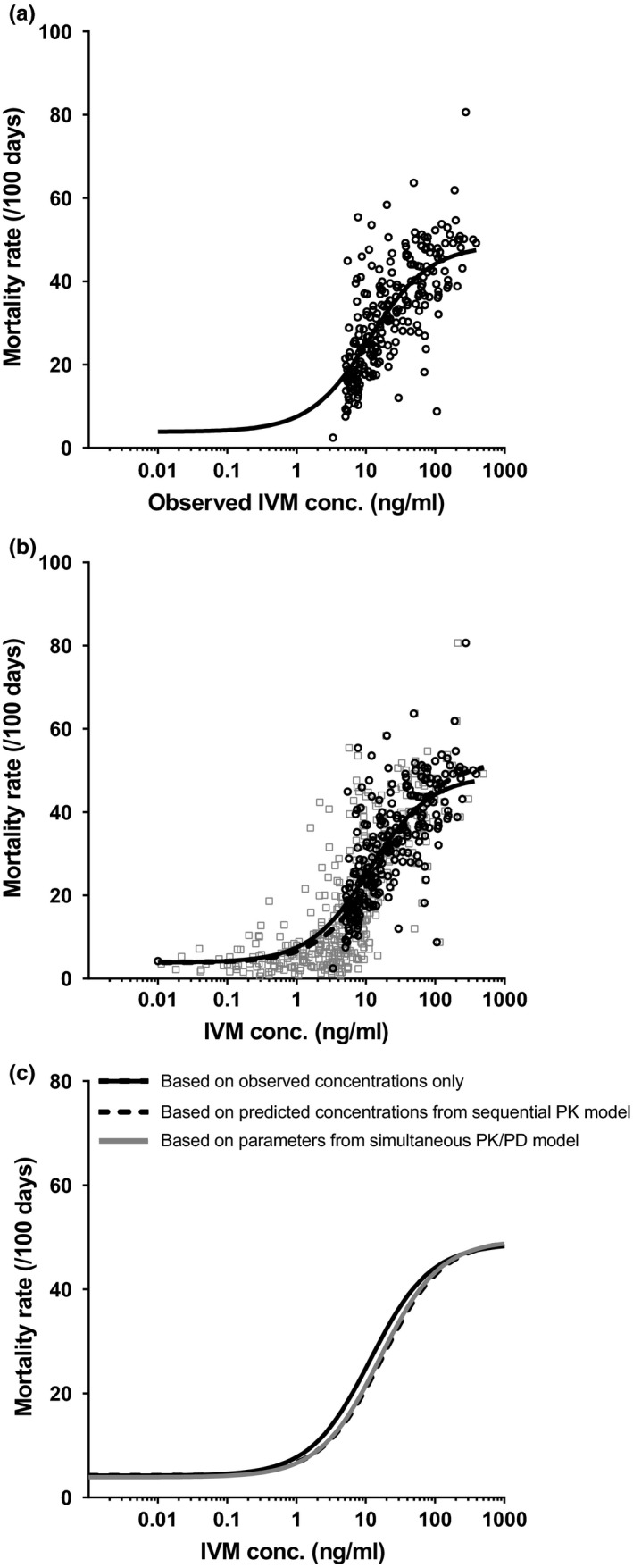
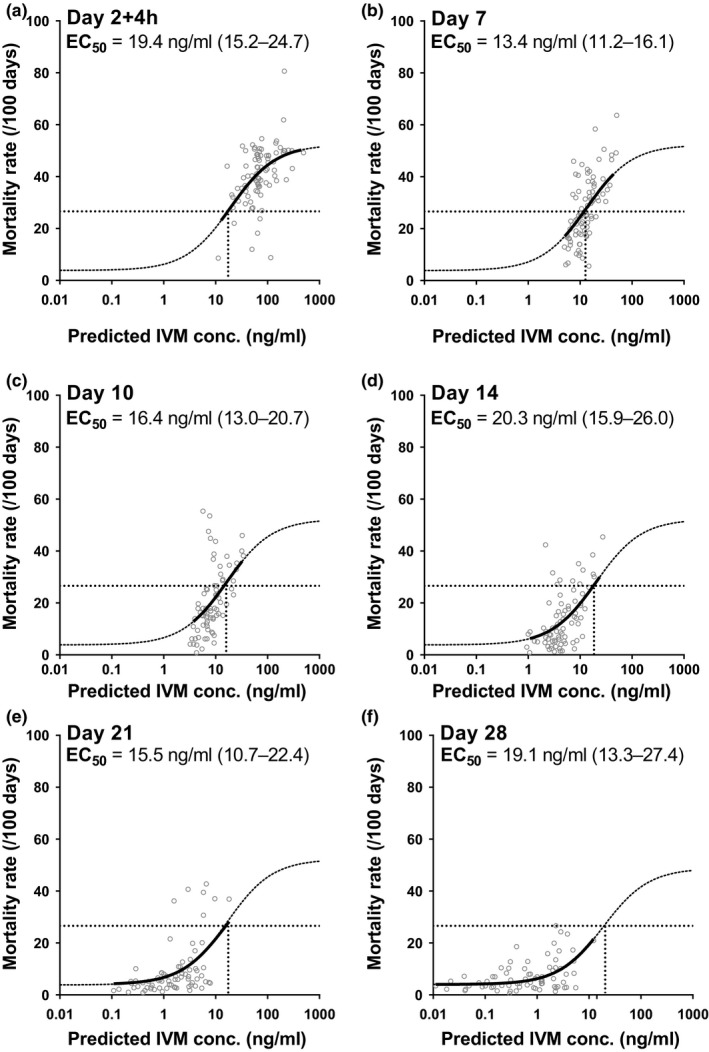
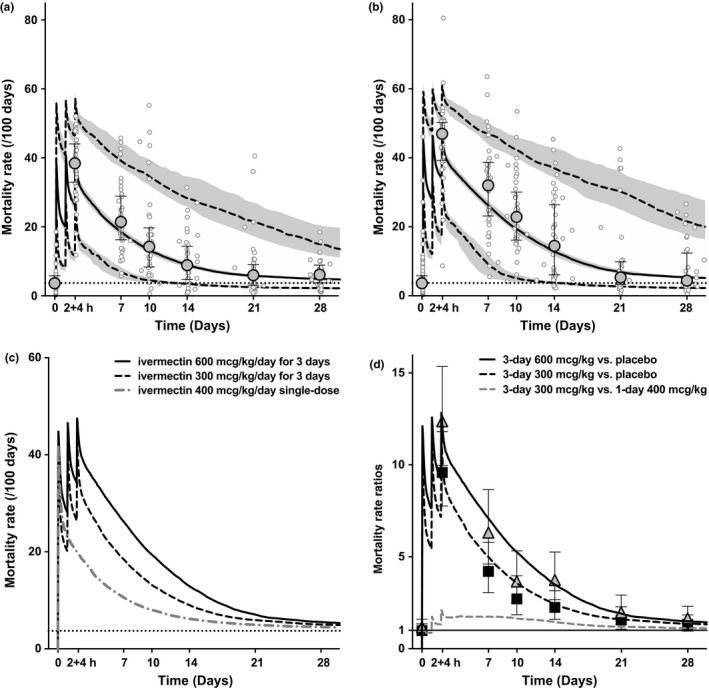
High-dose ivermectin, co-administered for 3 days with dihydroartemisinin-piperaquine (DP), killed mosquitoes feeding on individuals for at least 28 days posttreatment in a recent trial (IVERMAL), whereas 7 days was predicted pretrial. The current study assessed the relationship between ivermectin blood concentrations and the observed mosquitocidal effects against Anopheles gambiae s.s. Three days of ivermectin 0, 300, or 600 mcg/kg/day plus DP was randomly assigned to 141 adults with uncomplicated malaria in Kenya. During 28 days of follow-up, 1,393 venous and 335 paired capillary plasma samples, 850 mosquito-cluster mortality rates, and 524 QTcF-intervals were collected. Using pharmacokinetic/pharmacodynamic (PK/PD) modeling, we show a consistent correlation between predicted ivermectin concentrations and observed mosquitocidal-effects throughout the 28-day study duration, without invoking an unidentified mosquitocidal metabolite or drug-drug interaction. Ivermectin had no effect on piperaquine's PKs or QTcF-prolongation. The PK/PD model can be used to design new treatment regimens with predicted mosquitocidal effect. This methodology could be used to evaluate effectiveness of other endectocides.
© 2018 The Authors Clinical Pharmacology & Therapeutics published by Wiley Periodicals, Inc. on behalf of American Society for Clinical Pharmacology and Therapeutics.
Conflict of interest statement
The authors declared no competing interests for this work.
Figures
References
-
- Mwesigwa, J. et al Mass drug administration and reactive case detection for malaria elimination. ASTMH 2017 session. Am. J. Trop. Med. Hyg. 97(suppl. 5), 411–413 (2017).
-
- von Seidlein, L. et al Targeted malaria elimination in the greater Mekong subregion using mass drug administration. ECTMIH 2017 Session. Trop. Med. Int. Health 22, 394–396 (2017).
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
