

Measles outbreak propagated by children congregating at water collection points in Mayuge District, eastern Uganda, July - October, 2016
- PMID: 30126362
- PMCID: PMC6102928
- DOI: 10.1186/s12879-018-3304-5
Measles outbreak propagated by children congregating at water collection points in Mayuge District, eastern Uganda, July - October, 2016
Abstract
Background: On 12 October, 2016 a measles outbreak was reported in Mayuge District, eastern Uganda. We investigated the outbreak to determine its scope, identify risk factors for transmission, evaluate vaccination coverage and vaccine effectiveness, and recommend evidence-based control measures.
Methods: We defined a probable case as onset of fever (≥3 days) and generalized rash, plus ≥1 of the following: conjunctivitis, cough, and/or runny nose in a Mayuge District resident. A confirmed case was a probable case with measles-specific IgM (+) not explained by vaccination. We reviewed medical records and conducted active community case-finding. In a case-control investigation involving probable case-persons and controls matched by age and village, we evaluated risk factors for transmission for both cases and controls during the case-person's likely exposure period (i.e., 7-21 days prior to rash onset). We estimated vaccine effectiveness (VE) using the formula: VE ≈ (1-ORprotective) × 100. We calculated vaccination coverage using the percentage of controls vaccinated.
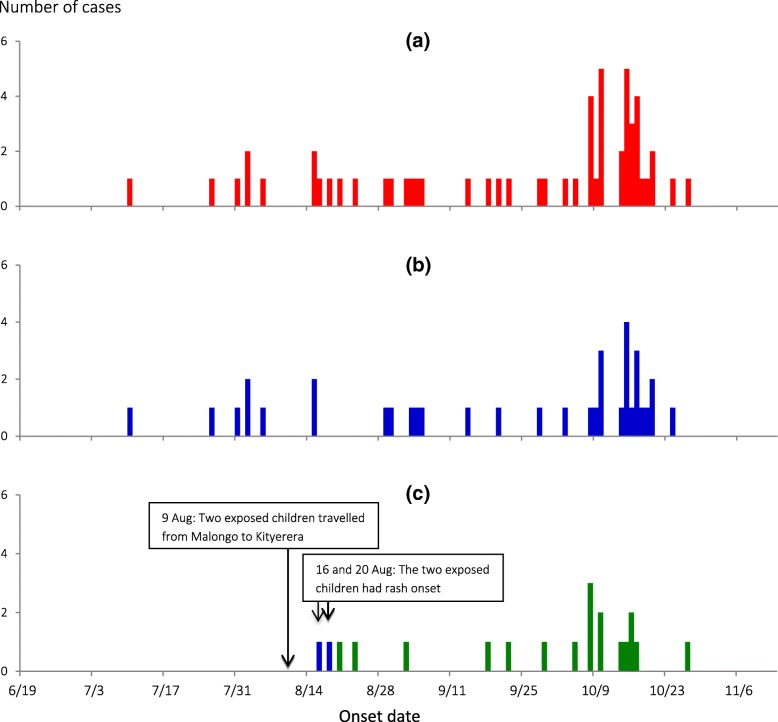
Results: We identified 62 probable case-persons (attack rate [AR] = 4.0/10,000), including 3 confirmed. Of all age groups, children < 5 years were the most affected (AR = 14/10,000). The epidemic curve showed a propagated outbreak. Thirty-two percent (13/41) of case-persons and 13% (21/161) of control-persons visited water-collection sites (by themselves or with parents) during the case-persons' likely exposure period (ORM-H = 5.0; 95% CI = 1.5-17). Among children aged 9-59 months, the effectiveness of the single-dose measles vaccine was 75% (95% CI = 25-92); vaccination coverage was 68% (95% CI = 61-76).
Conclusions: Low vaccine effectiveness, inadequate vaccination coverage and congregation at water collection points facilitated measles transmission in this outbreak. We recommended increasing measles vaccination coverage and restriction of children with signs and symptoms of measles from accessing public gatherings.
Keywords: Disease outbreaks; Measles; Risk factors; Uganda.
Conflict of interest statement
Ethics approval and consent to participate
The Ministry of Health of Uganda gave the directive and approval to investigate this outbreak. In agreement with the International Guidelines for Ethical Review of Epidemiological Studies by the Council for International Organizations of Medical Sciences (1991) and the Office of the Associate Director for Science, CDC/Uganda, determined that this activity was not human subjects research and its primary intent was public health practice or a disease control activity (specifically, epidemic or endemic disease control activity). Verbal informed consent was obtained from the participants before the start of each interview. For children less than 8 years, parental/legal guardian’s verbal informed consent was obtained on their behalf before start of each interview; for minors aged 8–18 years, verbal informed assent and parental/guardian’s informed verbal consent was obtained. For persons above 18 years, verbal informed consent was obtained before start of each interview. Verbal informed consent was obtained because it was impractical to obtained written consent as the affected community was illiterate and this investigation was conducted as part of an emergency outbreak investigation whose primary goal was to generate evidence to inform disease control as opposed to absolute human rights research. All participants were informed about the purpose and nature of the investigation and that their involvement was entirely voluntary; i.e. their refusal to answer any or all of the questions would not result in any negative consequences. Participants identified as patients were referred for free treatment at a nearby health facility. To protect participants’ confidentiality, personal information was de-identified during data analysis, and the interview forms were locked up.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- American Academy of Pediatrics . Measles. Redbook: 2009 Report of the Committee on Infectious Diseases. 28. ElK Grove Village: American Academy of Pediatrics; 2009.
-
- Griffin DE. Immune responses during measles virus infection. In: ter Meulen V, Billeter MA (eds): Measles Virus. Current topics in microbiology and immunology, Vol. 191. Springer-verlay, Berlin, Heildelbery 1995. p. 117–34. - PubMed
-
- Bloch AB, Orenstein WA, Ewing WM, Spain WH, Mallison GF, Herrmann KL, Hinman AR. Measles outbreak in a pediatric practice: airborne transmission in an office setting. Pediatrics. 1985;75(4):676–683. - PubMed
-
- CDC Vaccine preventable deaths and the global immunization vision and strategy, 2006-2015. MMWR. 2006;15(18):511–515. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
