

A practice change intervention to improve antenatal care addressing alcohol consumption by women during pregnancy: research protocol for a randomised stepped-wedge cluster trial
- PMID: 30126437
- PMCID: PMC6102816
- DOI: 10.1186/s13012-018-0806-x
A practice change intervention to improve antenatal care addressing alcohol consumption by women during pregnancy: research protocol for a randomised stepped-wedge cluster trial
Abstract
Background: Despite clinical guideline recommendations, implementation of antenatal care addressing alcohol consumption by pregnant women is limited. Implementation strategies addressing barriers to such care may be effective in increasing care provision. The aim of this study is to examine the effectiveness, cost and cost-effectiveness of a multi-strategy practice change intervention in increasing antenatal care addressing the consumption of alcohol by pregnant women.
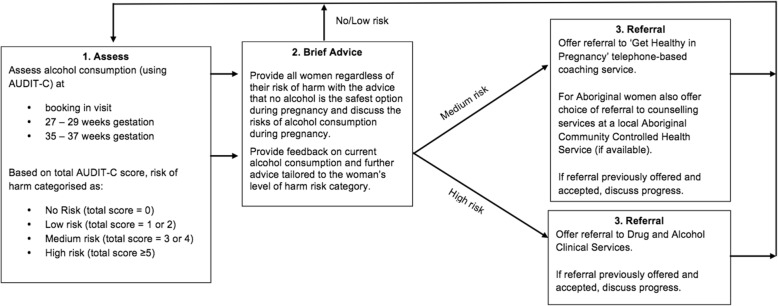
Methods: The study will be a randomised, stepped-wedge controlled trial conducted in three sectors in a health district in New South Wales, Australia. Stepped implementation of a practice change intervention will be delivered to sectors in a random order to support the introduction of a model of care for addressing alcohol consumption by pregnant women. A staged process was undertaken to develop the implementation strategies, which comprise of: leadership support, local clinical practice guidelines, electronic prompts and reminders, opinion leaders, academic detailing (audit and feedback), educational meetings and educational materials, and performance monitoring. Repeated cross-sectional outcome data will be gathered weekly across all sectors for the study duration. The primary outcome measures are the proportion of antenatal appointments at 'booking in', 27-28 weeks gestation and 35-36 weeks gestation for which women report (1) being assessed for alcohol consumption, (2) being provided with brief advice related to alcohol consumption during pregnancy, (3) receiving relevant care for addressing alcohol consumption during pregnancy, and (4) being assessed for alcohol consumption and receiving relevant care. Data on resources expended during intervention development and implementation will be collected. The proportion of women who report consuming alcohol since knowing they were pregnant will be measured as a secondary outcome.
Discussion: This will be the first randomised controlled trial to evaluate the effectiveness, cost and cost-effectiveness of implementation strategies in improving antenatal care that addresses alcohol consumption by pregnant women. If positive changes in clinical practice are found, this evidence will support health service adoption of implementation strategies to support improved antenatal care for this recognised risk to the health and wellbeing of the mother and child.
Trial registrations: Australian and New Zealand Clinical Trials Registry, No. ACTRN12617000882325 (date registered: 16/06/2017).
Keywords: Alcohol consumption; Antenatal care; Clinical practice change; Implementation; Maternal; Pregnancy; Protocol; Stepped-wedge trial.
Conflict of interest statement
Ethics approval and consent to participate
This study was approved by the Hunter New England Human Research Ethics Committee (16/11/16/4.07; 16/10/19/5.15), the Aboriginal Health and Medical Research Council (1236/16) and the University of Newcastle Human Research Ethics Committee (H-2017-0032; H-2016-0422).
Consent for publication
Not applicable.
Competing interests
Authors MK, ED, KC, BT, DT, LW, NB, MH, CA, KG and JW receive salary support from Hunter New England Clinical Services Nursing and Midwifery, which contributes funding to the project outlined in this protocol. Similarly, Author CR and Author SW receive salary support from the New South Wales Health Office of Preventive Health and the Foundation for Alcohol Research and Education, respectively. Both of these organisations also contribute funding to this project. All other authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures

Similar articles
-
Practice change intervention to improve antenatal care addressing alcohol consumption during pregnancy: a randomised stepped-wedge controlled trial.BMC Pregnancy Childbirth. 2022 Apr 21;22(1):345. doi: 10.1186/s12884-022-04646-7. BMC Pregnancy Childbirth. 2022. PMID: 35448996 Free PMC article. Clinical Trial.
-
Iterative delivery of an implementation support package to increase and sustain the routine provision of antenatal care addressing alcohol consumption during pregnancy: study protocol for a stepped-wedge cluster trial.BMJ Open. 2022 Jul 26;12(7):e063486. doi: 10.1136/bmjopen-2022-063486. BMJ Open. 2022. PMID: 35882461 Free PMC article.
-
Effect of implementation strategies on the routine provision of antenatal care addressing smoking in pregnancy: study protocol for a non-randomised stepped-wedge cluster controlled trial.BMJ Open. 2024 Apr 5;14(4):e076725. doi: 10.1136/bmjopen-2023-076725. BMJ Open. 2024. PMID: 38580367 Free PMC article.
-
Brief alcohol intervention to prevent drinking during pregnancy: an overview of research findings.Curr Opin Obstet Gynecol. 2009 Dec;21(6):496-500. doi: 10.1097/GCO.0b013e328332a74c. Curr Opin Obstet Gynecol. 2009. PMID: 19797951 Review.
-
Antenatal care trial interventions: a systematic scoping review and taxonomy development of care models.BMC Pregnancy Childbirth. 2017 Jan 6;17(1):8. doi: 10.1186/s12884-016-1186-3. BMC Pregnancy Childbirth. 2017. PMID: 28056877 Free PMC article.
Cited by
-
It takes a village: Influencing policy and practice to prevent alcohol use in pregnancy and promote better outcomes for individuals living with Fetal Alcohol Spectrum Disorder.Int J Popul Data Sci. 2022 Mar 2;6(1):1703. doi: 10.23889/ijpds.v6i1.1703. eCollection 2021. Int J Popul Data Sci. 2022. PMID: 35309099 Free PMC article.
-
The effects of maternal alcohol consumption during pregnancy on adverse fetal outcomes among pregnant women attending antenatal care at public health facilities in Gondar town, Northwest Ethiopia: a prospective cohort study.Subst Abuse Treat Prev Policy. 2021 Aug 26;16(1):64. doi: 10.1186/s13011-021-00401-x. Subst Abuse Treat Prev Policy. 2021. PMID: 34446055 Free PMC article.
-
Community Priority setting for Fetal Alcohol Spectrum Disorder Research in Australia.Int J Popul Data Sci. 2020 Dec 10;5(3):1359. doi: 10.23889/ijpds.v5i1.1359. Int J Popul Data Sci. 2020. PMID: 34036178 Free PMC article.
-
CASNET2: evaluation of an electronic safety netting cancer toolkit for the primary care electronic health record: protocol for a pragmatic stepped-wedge RCT.BMJ Open. 2020 Aug 24;10(8):e038562. doi: 10.1136/bmjopen-2020-038562. BMJ Open. 2020. PMID: 32843517 Free PMC article.
-
Clustering of smoking, alcohol consumption and weight gain in pregnancy: prevalence, care preferences and associated factors.BMC Pregnancy Childbirth. 2023 Nov 17;23(1):799. doi: 10.1186/s12884-023-06090-7. BMC Pregnancy Childbirth. 2023. PMID: 37978464 Free PMC article.
References
-
- National Health and Medical Research Council (NHMRC) Australian guidelines to reduce health risks from drinking alcohol. Canberra: Commonwealth of Australia; 2009.
-
- Butt P, Beirness D, Gliksman L, Paradis C, Stockwell T. Alcohol and health in Canada: a summary of evidence and guidelines for low risk drinking. Ottawa: Canadian Centre on Substance Abuse; 2011.
-
- The Danish National Board of Health . Healthy habits – before, during and after pregnancy. 1st English edition (translated from the 2nd Danish edition) Copenhagen South: The Danish National Board of Health and The Danish Committee for Health Education; 2010.
-
- O'Keeffe LM, Kearney PM, McCarthy FP, Khashan AS, Greene RA, North RA, Poston L, McCowan LM, Baker PN, Dekker GA, et al. Prevalence and predictors of alcohol use during pregnancy: findings from international multicentre cohort studies. BMJ Open. 2015;5:e006323. doi: 10.1136/bmjopen-2014-006323. - DOI - PMC - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
- APP1113032/National Health and Medical Research Council (AU)/International
- APP1113032/National Health and Medical Research Council (AU)/International
- APP1113032/National Health and Medical Research Council (AU)/International
- APP1113032/National Health and Medical Research Council (AU)/International
- APP1113032/National Health and Medical Research Council (AU)/International
- APP1113032/National Health and Medical Research Council (AU)/International
- APP1113032/National Health and Medical Research Council (AU)/International
- APP1113032/National Health and Medical Research Council (AU)/International
- APP1113032/National Health and Medical Research Council (AU)/International
- APP1113032/National Health and Medical Research Council (AU)/International
- APP1113032/National Health and Medical Research Council (AU)/International
- APP1113032/National Health and Medical Research Council (AU)/International
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
