

Trends over time in Escherichia coli bloodstream infections, urinary tract infections, and antibiotic susceptibilities in Oxfordshire, UK, 1998-2016: a study of electronic health records
- PMID: 30126643
- PMCID: PMC7612540
- DOI: 10.1016/S1473-3099(18)30353-0
Trends over time in Escherichia coli bloodstream infections, urinary tract infections, and antibiotic susceptibilities in Oxfordshire, UK, 1998-2016: a study of electronic health records
Abstract
Background: Escherichia coli bloodstream infections are increasing in the UK and internationally. The evidence base to guide interventions against this major public health concern is small. We aimed to investigate possible drivers of changes in the incidence of E coli bloodstream infection and antibiotic susceptibilities in Oxfordshire, UK, over the past two decades, while stratifying for time since hospital exposure.
Methods: In this observational study, we used all available data on E coli bloodstream infections and E coli urinary tract infections (UTIs) from one UK region (Oxfordshire) using anonymised linked microbiological data and hospital electronic health records from the Infections in Oxfordshire Research Database (IORD). We estimated the incidence of infections across a two decade period and the annual incidence rate ratio (aIRR) in 2016. We modelled the data using negative binomial regression on the basis of microbiological, clinical, and health-care-exposure risk factors. We investigated infection severity, 30-day all-cause mortality, and community and hospital amoxicillin plus clavulanic acid (co-amoxiclav) use to estimate changes in bacterial virulence and the effect of antimicrobial resistance on incidence.
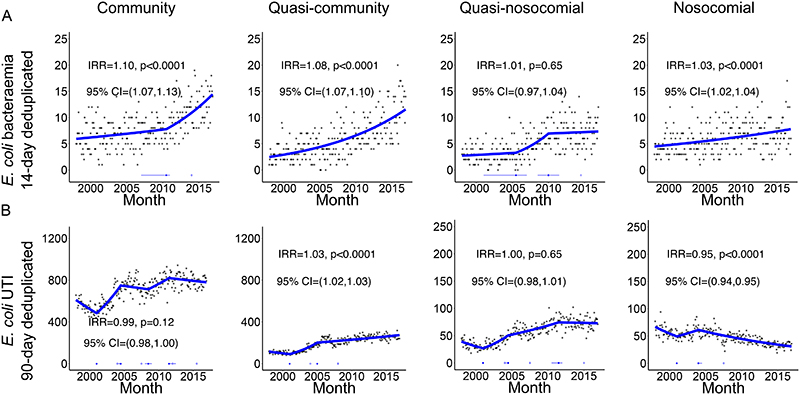
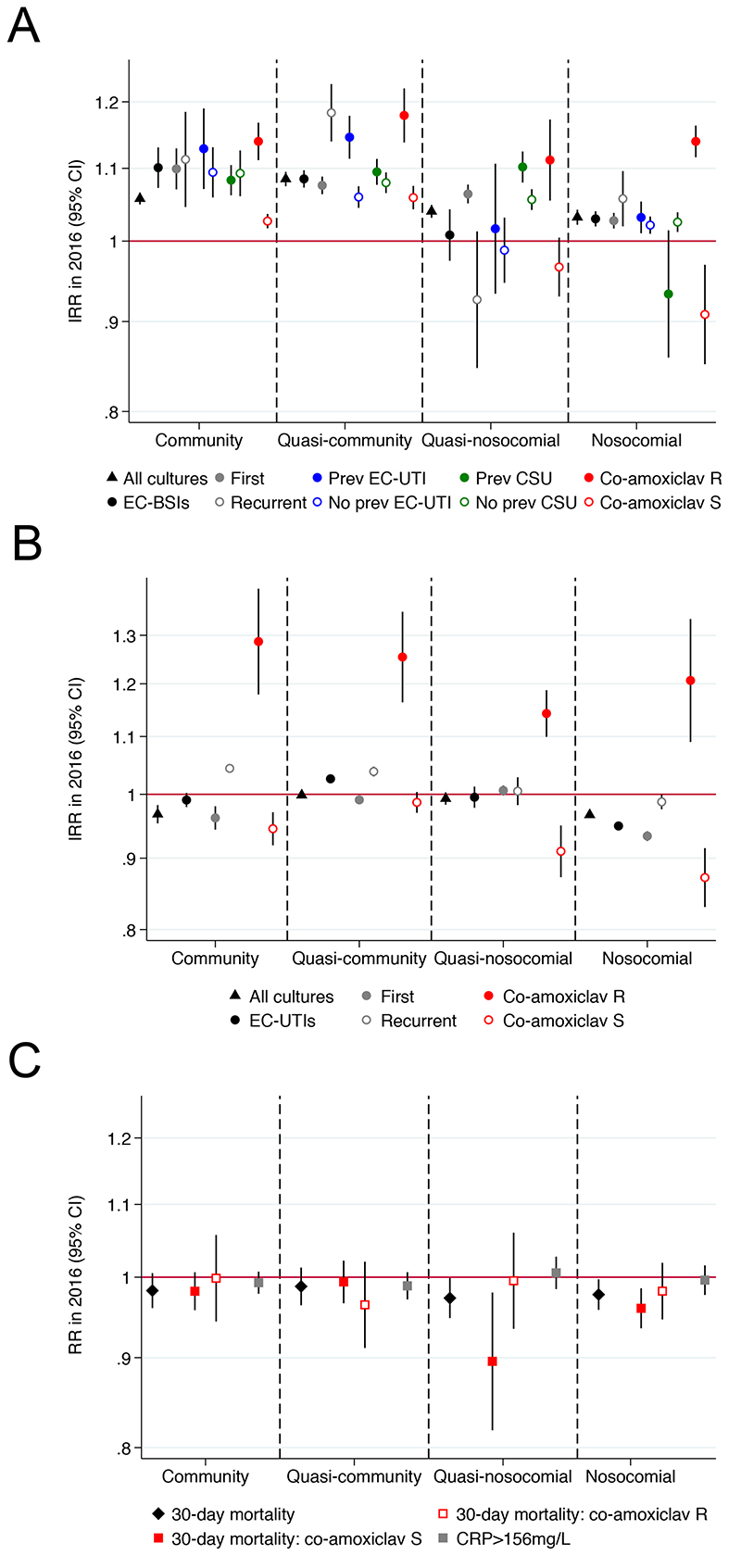
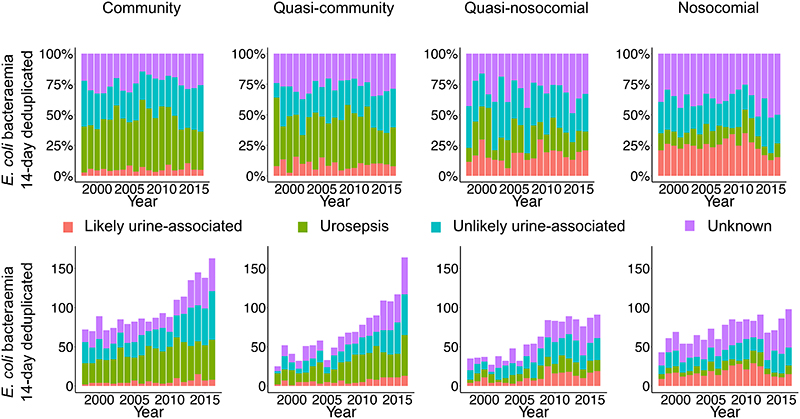
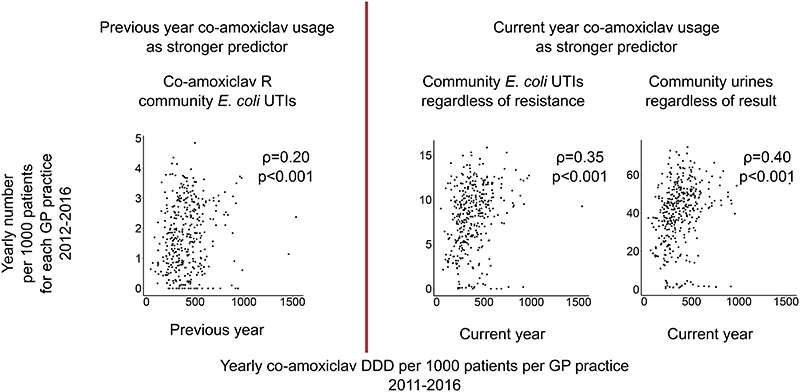
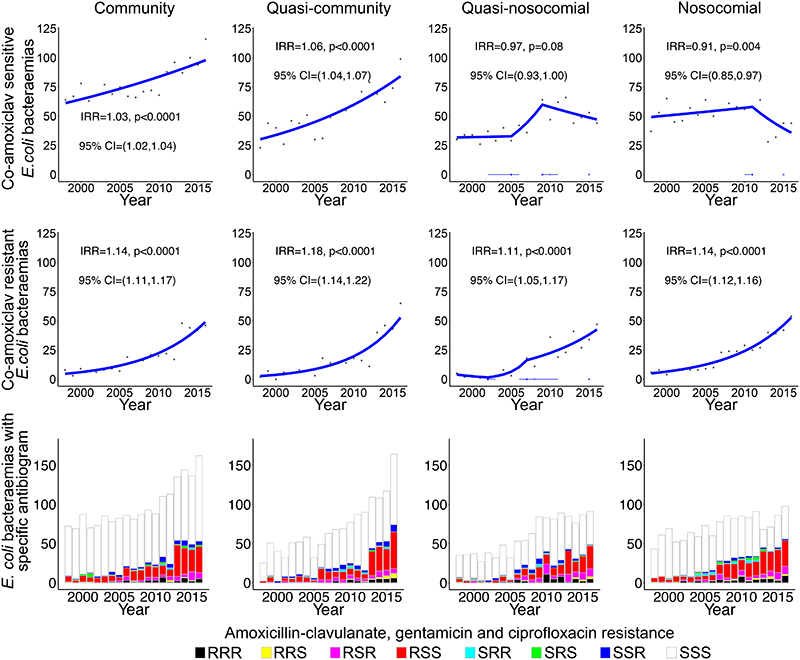
Findings: From Jan 1, 1998, to Dec 31, 2016, 5706 E coli bloodstream infections occurred in 5215 patients, and 228 376 E coli UTIs occurred in 137 075 patients. 1365 (24%) E coli bloodstream infections were nosocomial (onset >48 h after hospital admission), 1132 (20%) were quasi-nosocomial (≤30 days after discharge), 1346 (24%) were quasi-community (31-365 days after discharge), and 1863 (33%) were community (>365 days after hospital discharge). The overall incidence increased year on year (aIRR 1·06, 95% CI 1·05-1·06). In 2016, 212 (41%) of 515 E coli bloodstream infections and 3921 (28%) of 13 792 E coli UTIs were co-amoxiclav resistant. Increases in E coli bloodstream infections were driven by increases in community (aIRR 1·10, 95% CI 1·07-1·13; p<0·0001) and quasi-community (aIRR 1·08, 1·07-1·10; p<0·0001) cases. 30-day mortality associated with E coli bloodstream infection decreased over time in the nosocomial (adjusted rate ratio [RR] 0·98, 95% CI 0·96-1·00; p=0·03) group, and remained stable in the quasi-nosocomial (adjusted RR 0·98, 0·95-1·00; p=0·06), quasi-community (adjusted RR 0·99, 0·96-1·01; p=0·32), and community (adjusted RR 0·99, 0·96-1·01; p=0·21) groups. Mortality was, however, substantial at 14-25% across all hospital-exposure groups. Co-amoxiclav-resistant E coli bloodstream infections increased in all groups across the study period (by 11-18% per year, significantly faster than co-amoxiclav-susceptible E coli bloodstream infections; pheterogeneity<0·0001), as did co-amoxiclav-resistant E coli UTIs (by 14-29% per year; pheterogeneity<0·0001). Previous year co-amoxiclav use in primary-care facilities was associated with increased subsequent year community co-amoxiclav-resistant E coli UTIs (p=0·003).
Interpretation: Increases in E coli bloodstream infections in Oxfordshire are primarily community associated, with substantial co-amoxiclav resistance; nevertheless, we found little or no change in mortality. Focusing interventions on primary care facilities, particularly those with high co-amoxiclav use, could be effective in reducing the incidence of co-amoxiclav-resistant E coli bloodstream infections, in this region and more generally.
Funding: National Institute for Health Research.
Copyright © 2018 Elsevier Ltd. All rights reserved.
Conflict of interest statement
Dr. Peto reports grants from Wellcome Trust, grants from Medical Reserach Council, during the conduct of the study. All other authors report no conflicts of interest.
Figures
Comment in
-
Patterns in the epidemic of Escherichia coli bloodstream infection in Oxfordshire.Lancet Infect Dis. 2018 Oct;18(10):1057-1058. doi: 10.1016/S1473-3099(18)30418-3. Epub 2018 Aug 17. Lancet Infect Dis. 2018. PMID: 30126644 No abstract available.
References
-
- Public Health England. Polymicrobial Bacteraemia and Fungaemia in England, Wales and Northern Ireland 2014. 2015;9
-
- O’Neill J. Antimicrobial Resistance : Tackling a crisis for the health and wealth of nations. Rev Antimicrob Resist. 2014 December;:1–16.
-
- European Centre for Disease Prevention and Control. Surveillance of Antimicrobial Resistance in Europe: Annual Report of the European Antimicrobial Resistance Surveillance Network (EARS-Net) 2016.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
