

Continuous improvement in primary Debulking surgery for advanced ovarian cancer: Do increased complete gross resection rates independently lead to increased progression-free and overall survival?
- PMID: 30126704
- PMCID: PMC6247423
- DOI: 10.1016/j.ygyno.2018.08.014
Continuous improvement in primary Debulking surgery for advanced ovarian cancer: Do increased complete gross resection rates independently lead to increased progression-free and overall survival?
Abstract
Objectives: To assess complete gross resection (CGR) rates and survival outcomes in patients with advanced ovarian cancer who underwent primary debulking surgery (PDS) during a 13-year period in which specific changes to surgical paradigm were implemented.
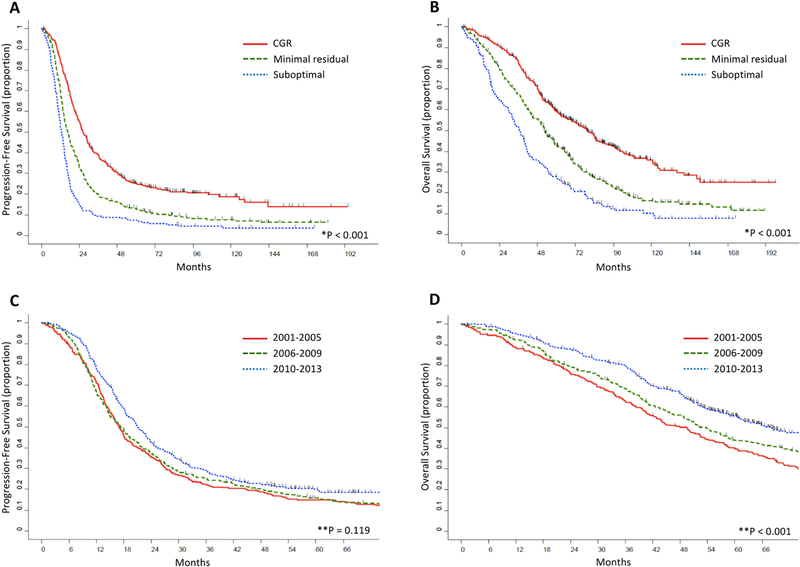
Methods: We identified all patients with stage IIIB-IV high-grade ovarian carcinoma who underwent PDS at our institution, with the intent of maximal cytoreduction, from 1/2001-12/2013. Patients were categorized by year of PDS based on the implementation of surgical changes to our approach to ovarian cancer debulking (Group 1, 2001-2005; Group 2, 2006-2009; Group 3, 2010-2013).
Results: Among 978 patients, 78% had stage IIIC disease and 89% had disease of serous histology. Carcinomatosis was found in 81%, and 60% had bulky upper abdominal disease (UAD). Compared to Group 1, those who underwent PDS during the latter 2 time periods had higher ASA scores (p < 0.001), higher-stage disease (p < 0.001), and more often had carcinomatosis (p = 0.015) and bulky UAD (p = 0.009). CGR rates for Groups 1-3 increased from 29% to 40% to 55%, respectively (p < 0.001). Five-year progression-free survival (PFS) rates increased over time (15%, 16%, and 20%, respectively; p = 0.199), as did 5-year overall survival (OS) rates (40%, 44%, and 56%, respectively; p < 0.001). On multivariable analysis, CGR was independently associated with PFS (p < 0.001) and OS (p < 0.001).
Conclusions: Despite higher-stage disease and greater tumor burden, CGR rates, PFS and OS for patients who underwent PDS increased over a 13-year period. Surgical paradigm shifts implemented specifically to achieve more complete surgical cytoreduction are likely the reason for these improvements.
Keywords: Complete gross resection; Ovarian cancer; Overall survival; Primary debulking surgery; Progression-free survival; Surgical paradigm.
Copyright © 2018 Elsevier Inc. All rights reserved.
Conflict of interest statement
Conflict of Interest Statement
Outside the submitted work, Dr. Dennis Chi is on the Medical Advisory Boards of Bovie Medical Co. and Verthermia Inc. The other authors have no conflicts of interest to disclose.
Figures
References
-
- Siegel RL, Miller KD, Jemal A. Cancer statistics, 2018. CA Cancer J Clin. 2018. January;68(1):7–30. PMID - PubMed
-
- Noone AM, Howlader N, Krapcho M, Miller D, Brest A, Yu M, Ruhl J, Tatalovich Z, Mariotto A, Lewis DR, Chen HS, Feuer EJ, Cronin KA (eds). SEER Cancer Statistics Review, 1975–2015, National Cancer Institute; Bethesda, MD, https://seer.cancer.gov/csr/1975_2015/, based on November 2017 SEER data submission, posted to the SEER web site, April 2018.
-
- Griffiths CT. Surgical resection of tumor bulk in the primary treatment of ovarian carcinoma. Natl Cancer Inst Monogr. 1975. October;42:101–4. PMID - PubMed
-
- Eisenkop SM, Friedman RL, Wang HJ. Complete cytoreductive surgery is feasible and maximizes survival in patients with advanced epithelial ovarian cancer: A prospective study. Gynecol Oncol 1998. May;69(2):103–8. PMID - PubMed
-
- Zivanovic O, Eisenhauer EL, Zhou Q, Iasonos A, Sabbatini P, Sonoda Y, Abu-Rustum NR, Barakat RR, Chi DS. The impact of bulky upper abdominal disease cephalad to the greater omentum on surgical outcome for stage IIIC epithelial ovarian, fallopian tube, and primary peritoneal cancer. Gynecol Oncol. 2008. February;108(2):287–92. PMID - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
