

De novo NAD+ biosynthetic impairment in acute kidney injury in humans
- PMID: 30127395
- PMCID: PMC6129212
- DOI: 10.1038/s41591-018-0138-z
De novo NAD+ biosynthetic impairment in acute kidney injury in humans
Abstract
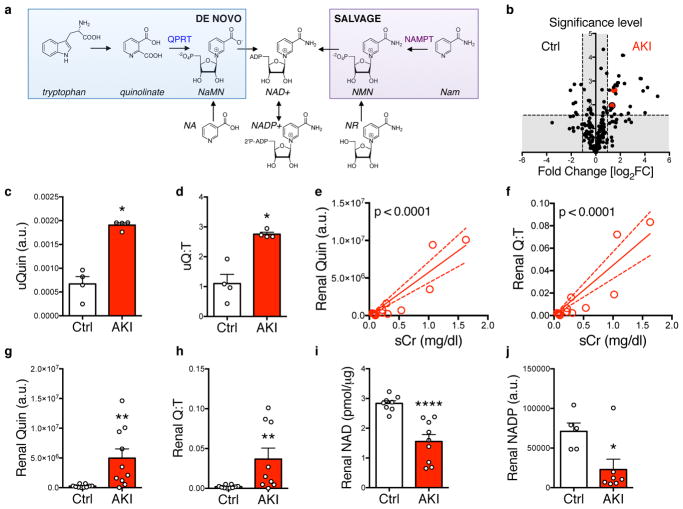
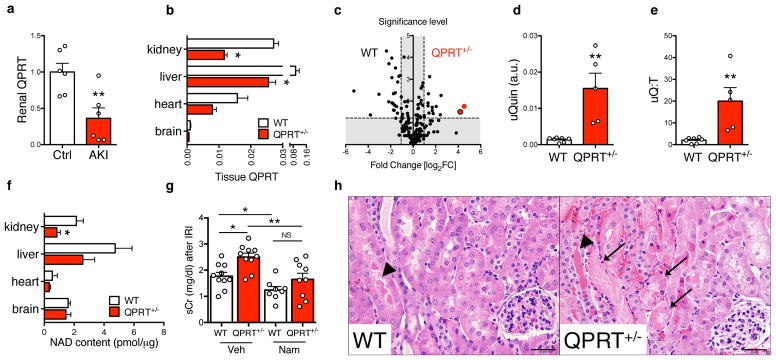
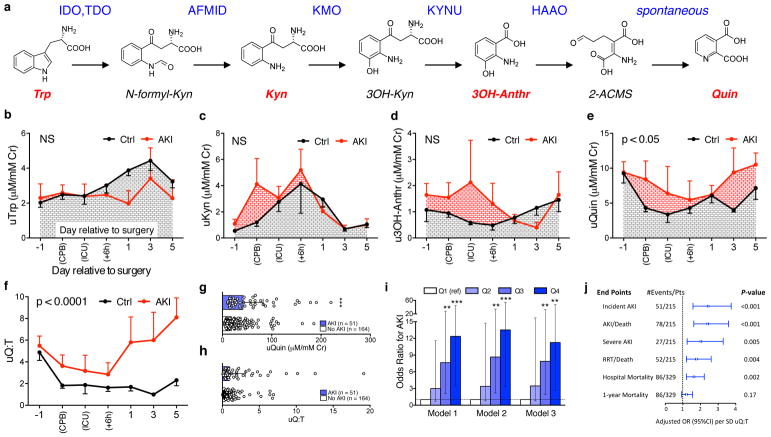
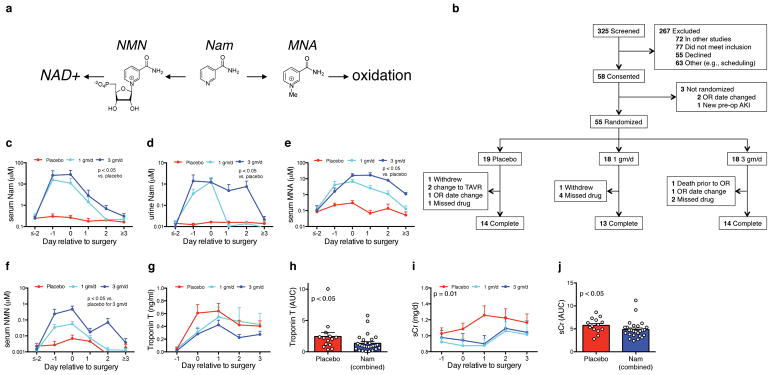
Nicotinamide adenine dinucleotide (NAD+) extends longevity in experimental organisms, raising interest in its impact on human health. De novo NAD+ biosynthesis from tryptophan is evolutionarily conserved yet considered supplanted among higher species by biosynthesis from nicotinamide (NAM). Here we show that a bottleneck enzyme in de novo biosynthesis, quinolinate phosphoribosyltransferase (QPRT), defends renal NAD+ and mediates resistance to acute kidney injury (AKI). Following murine AKI, renal NAD+ fell, quinolinate rose, and QPRT declined. QPRT+/- mice exhibited higher quinolinate, lower NAD+, and higher AKI susceptibility. Metabolomics suggested an elevated urinary quinolinate/tryptophan ratio (uQ/T) as an indicator of reduced QPRT. Elevated uQ/T predicted AKI and other adverse outcomes in critically ill patients. A phase 1 placebo-controlled study of oral NAM demonstrated a dose-related increase in circulating NAD+ metabolites. NAM was well tolerated and was associated with less AKI. Therefore, impaired NAD+ biosynthesis may be a feature of high-risk hospitalizations for which NAD+ augmentation could be beneficial.
Conflict of interest statement
S.M.P. is listed as an inventor on disclosures filed by Beth Israel Deaconess Medical Center pertaining to NAD+.
Figures
Comment in
-
Augmenting NAD+ may combat kidney stress.Nat Rev Nephrol. 2018 Nov;14(11):657. doi: 10.1038/s41581-018-0058-7. Nat Rev Nephrol. 2018. PMID: 30171208 No abstract available.
-
Modulating NAD+ metabolism to prevent acute kidney injury.Nat Med. 2018 Sep;24(9):1306-1307. doi: 10.1038/s41591-018-0181-9. Nat Med. 2018. PMID: 30177824 No abstract available.
-
The iNADequacy of renal cell metabolism: modulating NAD+ biosynthetic pathways to forestall kidney diseases.Kidney Int. 2019 Aug;96(2):264-267. doi: 10.1016/j.kint.2019.03.012. Kidney Int. 2019. PMID: 31331461 No abstract available.
References
-
- Collins PB, Chaykin S. The management of nicotinamide and nicotinic acid in the mouse. The Journal of biological chemistry. 1972;247:778–783. - PubMed
-
- Krehl WA, Teply LJ, Sarma PS, Elvehjem CA. Growth-Retarding Effect of Corn in Nicotinic Acid-Low Rations and Its Counteraction by Tryptophane. Science. 1945;101:489–490. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
