

TTP-like syndrome: novel concept and molecular pathogenesis of endotheliopathy-associated vascular microthrombotic disease
- PMID: 30127669
- PMCID: PMC6087012
- DOI: 10.1186/s12959-018-0174-4
TTP-like syndrome: novel concept and molecular pathogenesis of endotheliopathy-associated vascular microthrombotic disease
Abstract
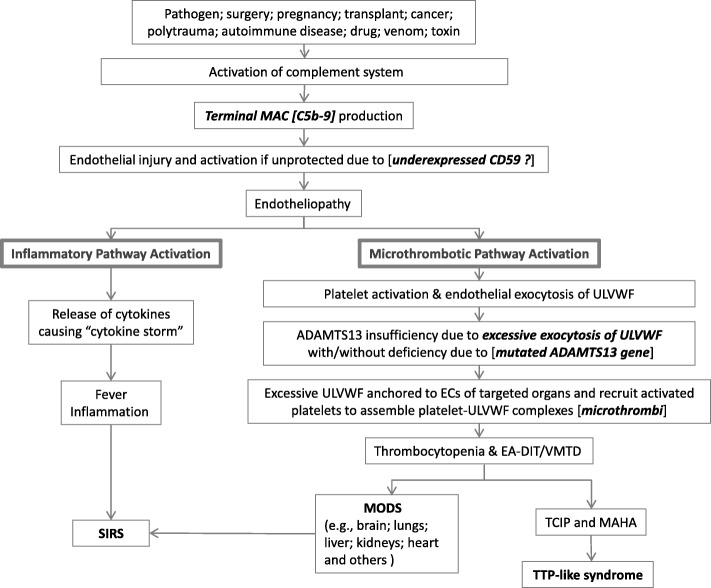
TTP is characterized by microangiopathic hemolytic anemia and thrombocytopenia associated with brain and kidney dysfunction. It occurs due to ADAMTS13 deficiency. TTP-like syndrome occurs in critically ill patients with the similar hematologic changes and additional organ dysfunction syndromes. Vascular microthrombotic disease (VMTD) includes both TTP and TTP-like syndrome because their underlying pathology is the same disseminated intravascular microthrombosis (DIT). Microthrombi are composed of platelet-unusually large von Willebrand factor multimers (ULVWF) complexes. TTP occurs as a result of accumulation of circulating ULVWF secondary to ADAMTS13 deficiency. This protease deficiency triggers microthrombogenesis, leading to "microthrombi" formation in microcirculation. Unlike TTP, TTP-like syndrome occurs in critical illnesses due to complement activation. Terminal C5b-9 complex causes channel formation to endothelial membrane, leading to endotheliopathy, which activates two different molecular pathways (i.e., inflammatory and microthrombotic). Activation of inflammatory pathway triggers inflammation. Activation of microthrombotic pathway promotes platelet activation and excessive endothelial exocytosis of ULVWF from endothelial cells (ECs). Overexpressed and uncleaved ULVWF become anchored to ECs as long elongated strings to recruit activated platelets, and assemble "microthrombi". In TTP, circulating microthrombi typically be lodged in microvasculature of the brain and kidney, but in TTP-like syndrome, microthrombi anchored to ECs of organs such as the lungs and liver as well as the brain and kidneys, leading to multiorgan dysfunction syndrome. TTP occurs as hereditary or autoimmune disease and is the phenotype of ADAMTS13 deficiency-associated VMTD. But TTP-like syndrome is hemostatic disorder occurring in critical illnesses and is the phenotype of endotheliopathy-associated VMTD. Thus, this author's contention is TTP and TTP-like syndrome are two distinctly different disorders with dissimilar underlying pathology and pathogenesis.
Keywords: ADAMTS13; Complement; Disseminated intravascular coagulation (DIC); Disseminated intravascular microthrombosis (DIT); Endotheliopathy; Microthrombogenesis; TTP-like syndrome; Thrombotic thrombocytopenic purpura (TTP); Unusually large von Willbrand factor multimers (ULVWF); Vascular microthrombotic disease (VMTD).
Conflict of interest statement
Board certified hematologist and hematopathologist, retired professor of medicine in the University of California Irvine School of Medicine, and retired professor of medicine in the Wright State University of School of Medicine. Not applicable. Not applicable. The author declares that he have no competing interests. Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Chang JC. A Thought on Possible Pathogenesis of Ebola Viral Hemorrhagic Disease and Potential Treatments: Could it Be Thrombotic Thrombocytopenic Purpura-like Syndrome? Ther Apher Dial. 2015;20:93–98. - PubMed
-
- Chang JC. Thrombocytopenia in critically ill patients due to vascular microthrombotic disease: pathogenesis based on “two activation theory of the endothelium”. Vascul Dis Ther. 2017;2:1–7.
-
- Chang JC. Molecular pathogenesis of STEC-HUS caused by endothelial heterogeneity and unprotected complement activation, leading to endotheliopathy and impaired ADAMTS13 activity: based on two-activation theory of the endothelium and vascular microthrombotic disease. Nephrol Renal Dis. 2017;2:1–8.
-
- Chauhan AK, Goerge T, Schneider SW, Wagner DD. Formation of platelet strings and microthrombi in the presence of ADAMTS-13 inhibitor does not require P-selectin or beta3 integrin. J Thromb Haemost. 2007;5:583–589. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
