

Excess mortality and cardiovascular disease in young adults with type 1 diabetes in relation to age at onset: a nationwide, register-based cohort study
- PMID: 30129464
- PMCID: PMC6828554
- DOI: 10.1016/S0140-6736(18)31506-X
Excess mortality and cardiovascular disease in young adults with type 1 diabetes in relation to age at onset: a nationwide, register-based cohort study
Abstract
Background: People with type 1 diabetes are at elevated risk of mortality and cardiovascular disease, yet current guidelines do not consider age of onset as an important risk stratifier. We aimed to examine how age at diagnosis of type 1 diabetes relates to excess mortality and cardiovascular risk.
Methods: We did a nationwide, register-based cohort study of individuals with type 1 diabetes in the Swedish National Diabetes Register and matched controls from the general population. We included patients with at least one registration between Jan 1, 1998, and Dec 31, 2012. Using Cox regression, and with adjustment for diabetes duration, we estimated the excess risk of all-cause mortality, cardiovascular mortality, non-cardiovascular mortality, acute myocardial infarction, stroke, cardiovascular disease (a composite of acute myocardial infarction and stroke), coronary heart disease, heart failure, and atrial fibrillation. Individuals with type 1 diabetes were categorised into five groups, according to age at diagnosis: 0-10 years, 11-15 years, 16-20 years, 21-25 years, and 26-30 years.
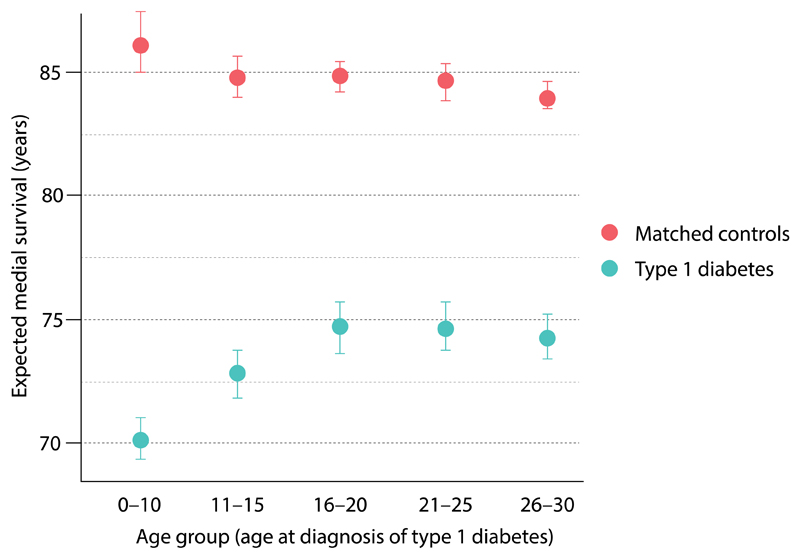
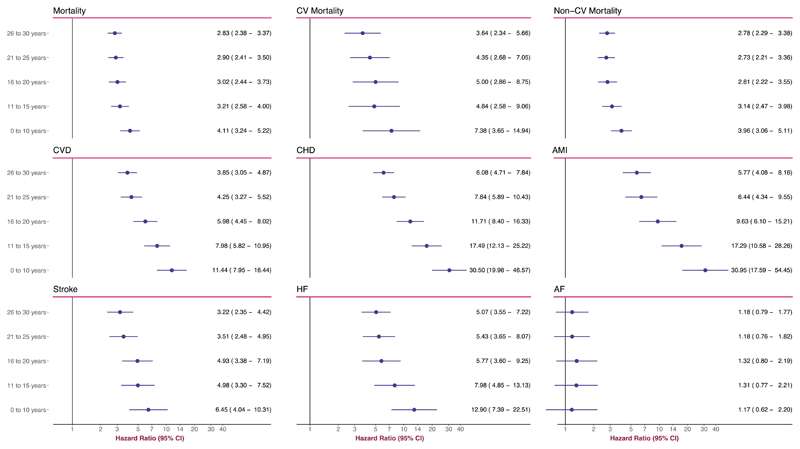
Findings: 27 195 individuals with type 1 diabetes and 135 178 matched controls were selected for this study. 959 individuals with type 1 diabetes and 1501 controls died during follow-up (median follow-up was 10 years). Patients who developed type 1 diabetes at 0-10 years of age had hazard ratios of 4·11 (95% CI 3·24-5·22) for all-cause mortality, 7·38 (3·65-14·94) for cardiovascular mortality, 3·96 (3·06-5·11) for non-cardiovascular mortality, 11·44 (7·95-16·44) for cardiovascular disease, 30·50 (19·98-46·57) for coronary heart disease, 30·95 (17·59-54·45) for acute myocardial infarction, 6·45 (4·04-10·31) for stroke, 12·90 (7·39-22·51) for heart failure, and 1·17 (0·62-2·20) for atrial fibrillation. Corresponding hazard ratios for individuals who developed type 1 diabetes aged 26-30 years were 2·83 (95% CI 2·38-3·37) for all-cause mortality, 3·64 (2·34-5·66) for cardiovascular mortality, 2·78 (2·29-3·38) for non-cardiovascular mortality, 3·85 (3·05-4·87) for cardiovascular disease, 6·08 (4·71-7·84) for coronary heart disease, 5·77 (4·08-8·16) for acute myocardial infarction, 3·22 (2·35-4·42) for stroke, 5·07 (3·55-7·22) for heart failure, and 1·18 (0·79-1·77) for atrial fibrillation; hence the excess risk differed by up to five times across the diagnosis age groups. The highest overall incidence rate, noted for all-cause mortality, was 1·9 (95% CI 1·71-2·11) per 100 000 person-years for people with type 1 diabetes. Development of type 1 diabetes before 10 years of age resulted in a loss of 17·7 life-years (95% CI 14·5-20·4) for women and 14·2 life-years (12·1-18·2) for men.
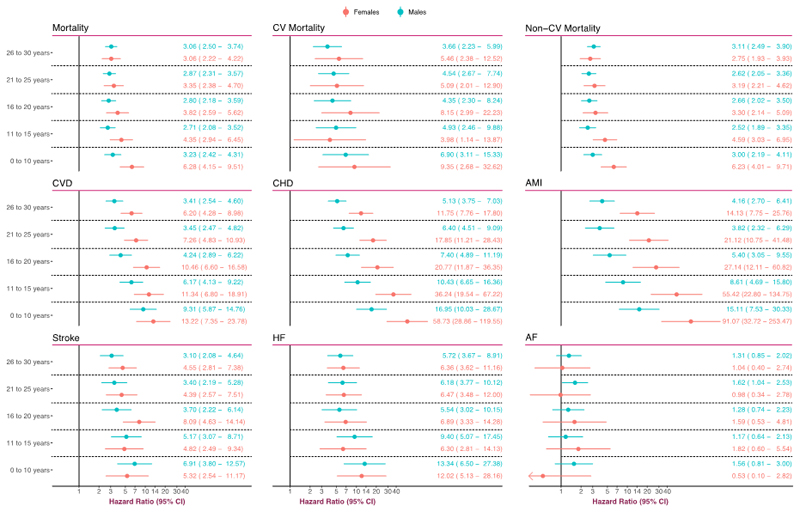
Interpretation: Age at onset of type 1 diabetes is an important determinant of survival, as well as all cardiovascular outcomes, with highest excess risk in women. Greater focus on cardioprotection might be warranted in people with early-onset type 1 diabetes.
Funding: Swedish Heart and Lung Foundation.
Copyright © 2018 Elsevier Ltd. All rights reserved.
Conflict of interest statement
NS has consulted for Boehringer Ingelheim, Novo Nordisk, Janssen and Eli Lilly, and received grant support from AstraZeneca. BE has received personal fees (advisory panels and/or consultant) from Amgen, AstraZeneca, Boerhringer Ingelheim, Eli Lilly, Merck Sharp & Dohme, Mundipharma, Navamedic, Novo Nordisk, and RLS Global outside the submitted work, and grants from Sanofi outside the submitted work. SG has received personal fees (lecture fees and research grants) from AstraZeneca, Boerhringer Ingelheim, Eli Lilly, Merck Sharp & Dohme, Novo Nordisk, Sanofi outside the submitted work. Ar.R has received personal fees from Novo Nordisk.
Figures
Comment in
-
Age at type 1 diabetes onset: a new risk factor and call for focused treatment.Lancet. 2018 Aug 11;392(10146):453-454. doi: 10.1016/S0140-6736(18)31811-7. Epub 2018 Aug 9. Lancet. 2018. PMID: 30129445 No abstract available.
-
Excess mortality and cardiovascular disease risk in type 1 diabetes.Lancet. 2019 Mar 9;393(10175):984-985. doi: 10.1016/S0140-6736(18)33050-2. Lancet. 2019. PMID: 30860047 No abstract available.
-
Excess mortality and cardiovascular disease risk in type 1 diabetes - Authors' reply.Lancet. 2019 Mar 9;393(10175):985-986. doi: 10.1016/S0140-6736(18)33061-7. Lancet. 2019. PMID: 30860049 No abstract available.
-
Excess mortality and cardiovascular disease risk in type 1 diabetes.Lancet. 2019 Mar 9;393(10175):985. doi: 10.1016/S0140-6736(18)33047-2. Lancet. 2019. PMID: 30860050 No abstract available.
References
-
- Gale EAM. The rise of childhood type 1 diabetes in the 20th century. Diabetes. 2002;51(12):3353–61. - PubMed
-
- Rawshani A, Rawshani A, Franzén S, et al. Mortality and Cardiovascular Disease in Type 1 and Type 2 Diabetes. The New England journal of medicine. 2017;376(15):1407–18. - PubMed
-
- Lind M, Svensson A-M, Kosiborod M, et al. Glycemic Control and Excess Mortality in Type 1 Diabetes. The New England journal of medicine. 2014;371(21):1972–82. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
