

Epicardial Fat Distribution Assessed with Cardiac CT in Arrhythmogenic Right Ventricular Dysplasia/Cardiomyopathy
- PMID: 30129902
- PMCID: PMC6276062
- DOI: 10.1148/radiol.2018180224
Epicardial Fat Distribution Assessed with Cardiac CT in Arrhythmogenic Right Ventricular Dysplasia/Cardiomyopathy
Abstract
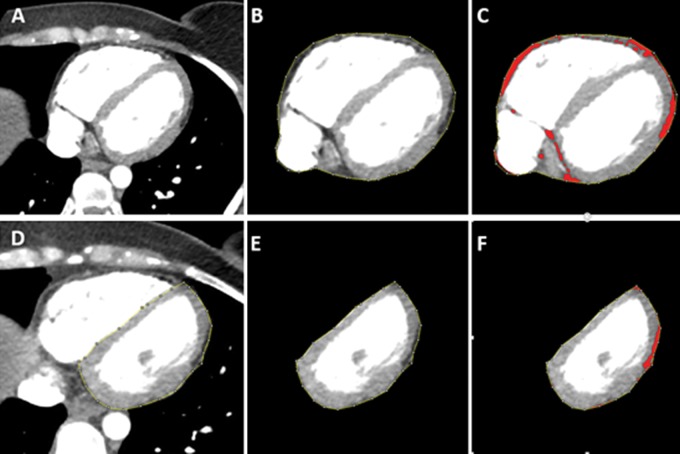
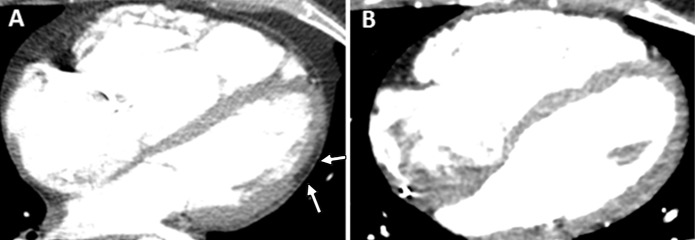
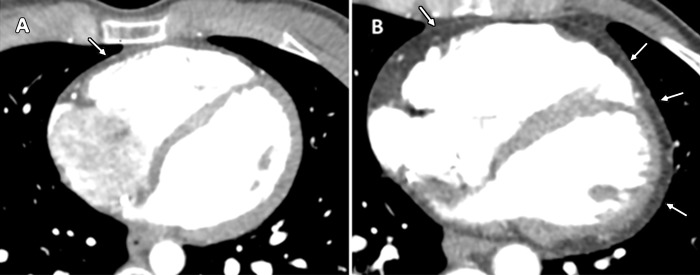
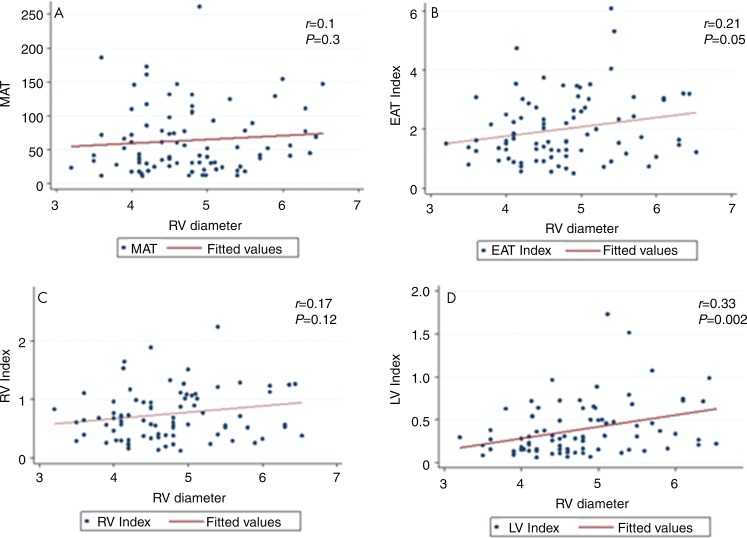
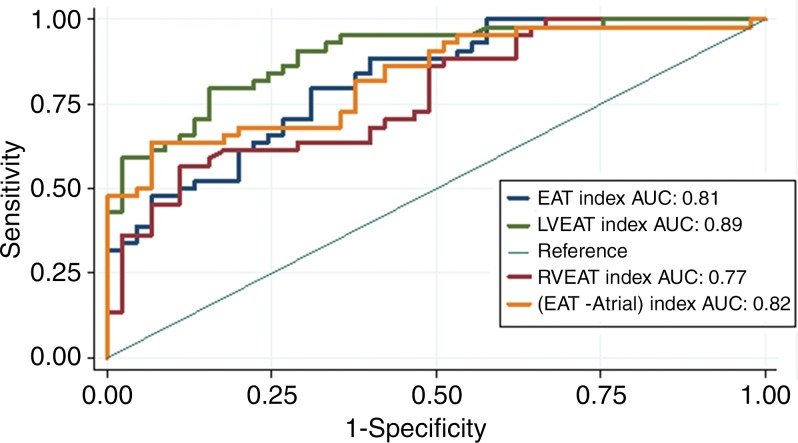
Purpose To compare epicardial fat in patients with arrhythmogenic right ventricular dysplasia/cardiomyopathy (ARVD/C) with that in healthy subjects. Materials and Methods In this retrospective study, cardiac CT scans in 44 patients with ARVD/C (mean age, 39 years ± 12; 23 men) were compared with those in 45 control group participants between January 2008 and July 2015. Volumes of intrathoracic adipose tissue, mediastinal adipose tissue (MAT), and total epicardial adipose tissue (EAT) were quantified. EAT was subdivided into three regions-right ventricular (RV) EAT, left ventricular (LV) EAT, and peri-atrial EAT (atrial EAT)-and normalized to MAT for all regions. Logistic regression and receiver operating characteristic analysis were performed to evaluate the association between epicardial fat with the diagnosis of ARVD/C. Results Total EAT volume was higher in patients with ARVD/C than in healthy control group participants (median, 98 mL vs 76 mL, respectively; P = .04). Regionally, LV and RV EAT volumes were higher in patients with ARVD/C than in control group participants, most notably when indexed to MAT (median LV EAT index: 0.49 vs 0.15, respectively; median RV EAT index: 0.91 vs 0.52; P ˂ .0005 for both). The optimal cutoff for diagnosis of ARVD/C was an LV EAT index of 0.24, with a sensitivity and specificity of 91% and 71%, respectively. Atrial EAT volume and total intrathoracic adipose tissue volume were not different between groups. RV diameter showed a positive correlation with total EAT index and LV EAT index (r = 0.21, P = .05 and r = 0.33, P = .002, respectively). Conclusion Higher amounts of right ventricular and left ventricular epicardial fat are found in hearts with arrhythmogenic right ventricular dysplasia/cardiomyopathy, particularly adjacent to the left ventricle, which correlates with disease severity and helps differentiate patients from healthy subjects. © RSNA, 2018 Online supplemental material is available for this article.
Figures
References
-
- Dalal D, Nasir K, Bomma C, et al. Arrhythmogenic right ventricular dysplasia: a United States experience. Circulation 2005;112(25):3823–3832. - PubMed
-
- Hulot JS, Jouven X, Empana JP, Frank R, Fontaine G. Natural history and risk stratification of arrhythmogenic right ventricular dysplasia/cardiomyopathy. Circulation 2004;110(14):1879–1884. - PubMed
-
- Calkins H, Tandri H. Left ventricular involvement in ARVD/C: is it time to readjust our views? Circ Arrhythm Electrophysiol 2015;8(6):1311–1312. - PubMed
-
- Bomma C, Dalal D, Tandri H, et al. Evolving role of multidetector computed tomography in evaluation of arrhythmogenic right ventricular dysplasia/cardiomyopathy. Am J Cardiol 2007;100(1):99–105. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
