

Moving Toward Individualized Medicine for Uterine Leiomyomas
- PMID: 30130343
- PMCID: PMC6153058
- DOI: 10.1097/AOG.0000000000002785
Moving Toward Individualized Medicine for Uterine Leiomyomas
Abstract
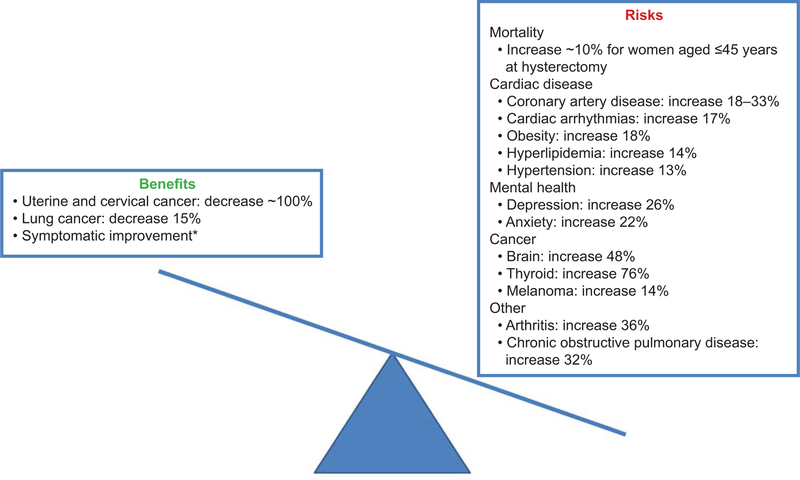
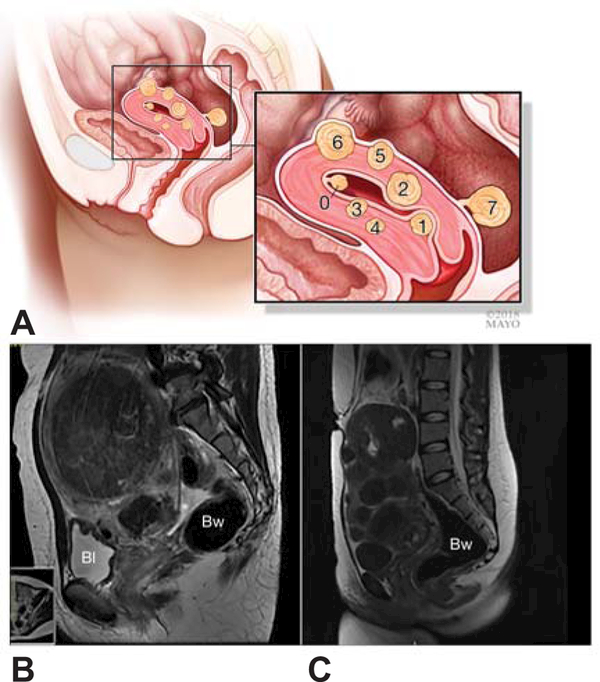
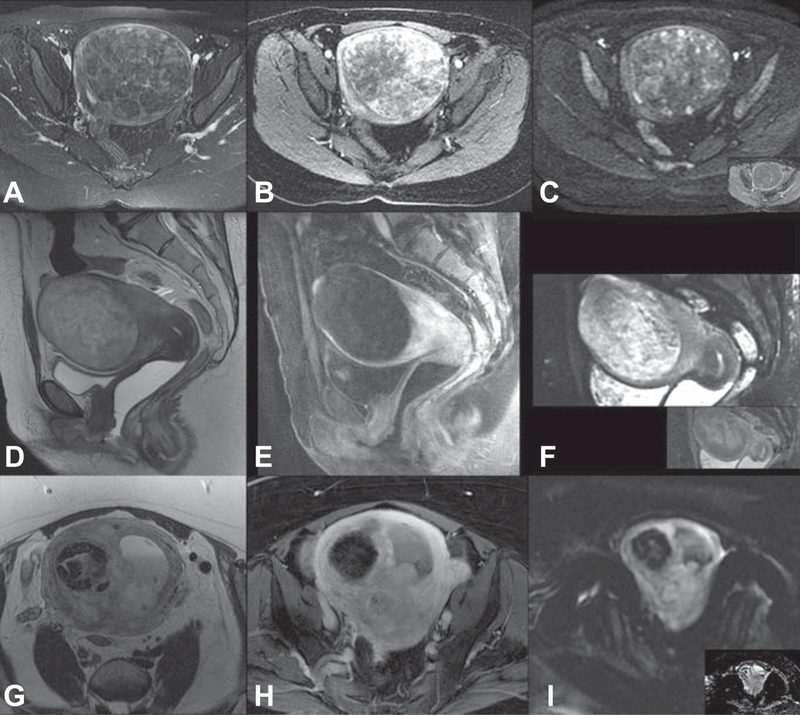
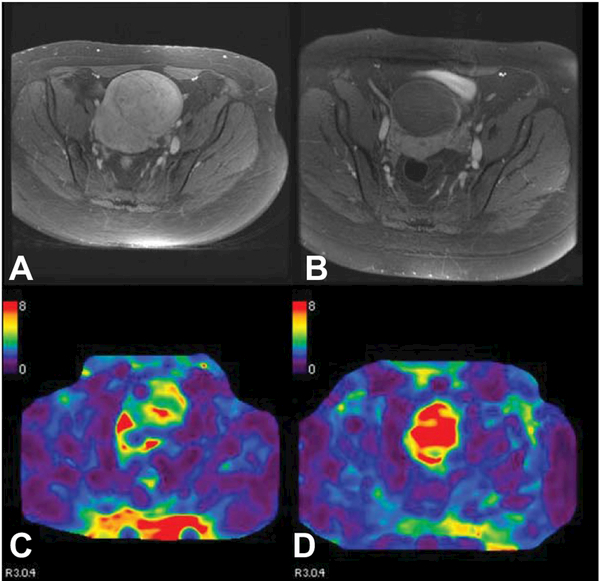
Uterine leiomyomas are common and life-altering for many women. Despite a wide range of symptoms, varying characteristics of the uterus and the leiomyomas themselves, and many alternatives, hysterectomy accounts for almost three fourths of all surgical therapy, yet there is increasing evidence for a variety of procedural therapies for symptomatic leiomyomas and a new generation of medical therapies under development. With increasing evidence of long-term risk from hysterectomy and new data regarding leiomyoma biology, individualized medical approaches to leiomyomas are likely in the near future. Key biological attributes that influence this disease process are common driver mutations and the new appreciation of the interaction of smooth muscle cells and fibroblasts. Additionally, the interaction between cell types and steroid hormone responsiveness likely plays a role in pathogenesis that can be leveraged in individualized therapy. However, given the independent clonal nature of leiomyomas within the same uterus, moving in the direction of biopsies for individual leiomyomas to understand the biology is unlikely to be fruitful. Use of advanced imaging will likely continue to evolve not only to accurately predict malignant disease, including sarcomas, but to predict leiomyoma subtypes, response to therapy, or both. We predict the continued evolution of therapy from excisional or interventional therapies to medical therapies and ultimately prediction of at-risk individuals. Ideally, individualized therapies will offer primary prevention for women at high risk of leiomyomas and secondary prevention after initial treatment.
Figures
References
-
- Stewart EA, Laughlin-Tommaso SK, Catherino WH, Lalitkumar S, Gupta D, Vollenhoven B. Uterine fibroids. Nat Rev Dis Primers 2016. June 23;2:16043. - PubMed
-
- Day Baird D, Dunson DB, Hill MC, Cousins D, Schectman JM. High cumulative incidence of uterine leiomyoma in black and white women: ultrasound evidence. Am J Obstet Gynecol 2003. January;188(1):100-7. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
