

Using routinely collected laboratory data to identify high rifampicin-resistant tuberculosis burden communities in the Western Cape Province, South Africa: A retrospective spatiotemporal analysis
- PMID: 30130377
- PMCID: PMC6103505
- DOI: 10.1371/journal.pmed.1002638
Using routinely collected laboratory data to identify high rifampicin-resistant tuberculosis burden communities in the Western Cape Province, South Africa: A retrospective spatiotemporal analysis
Abstract
Background: South Africa has the highest tuberculosis incidence globally (781/100,000), with an estimated 4.3% of cases being rifampicin resistant (RR). Control and elimination strategies will require detailed spatial information to understand where drug-resistant tuberculosis exists and why it persists in those communities. We demonstrate a method to enable drug-resistant tuberculosis monitoring by identifying high-burden communities in the Western Cape Province using routinely collected laboratory data.
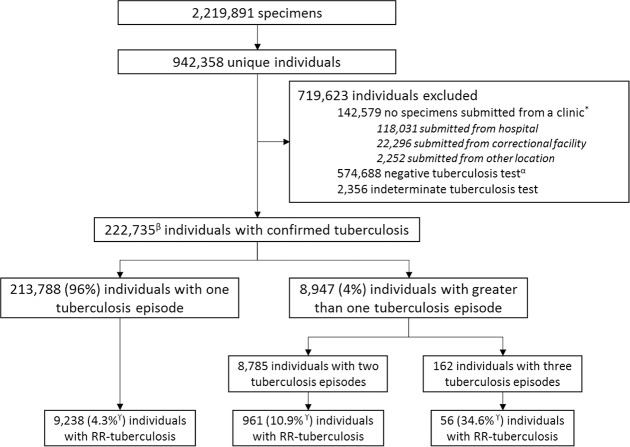
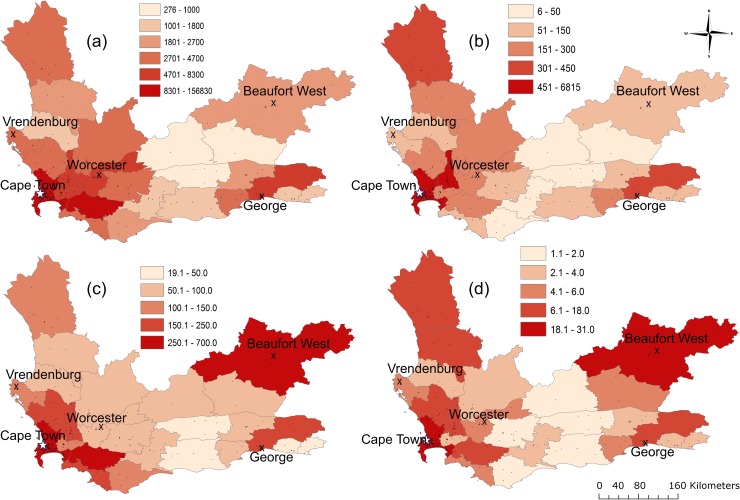
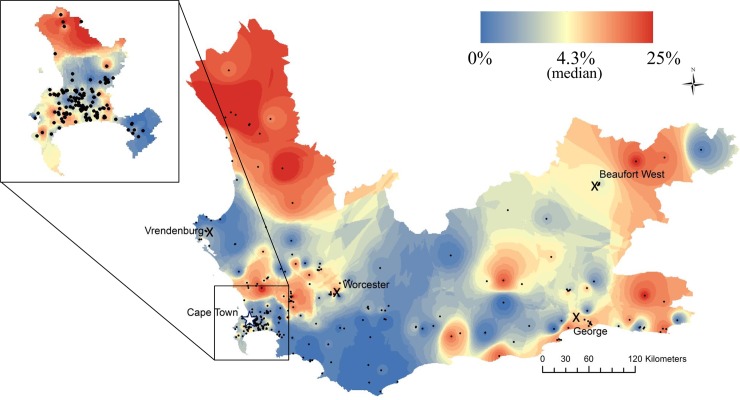
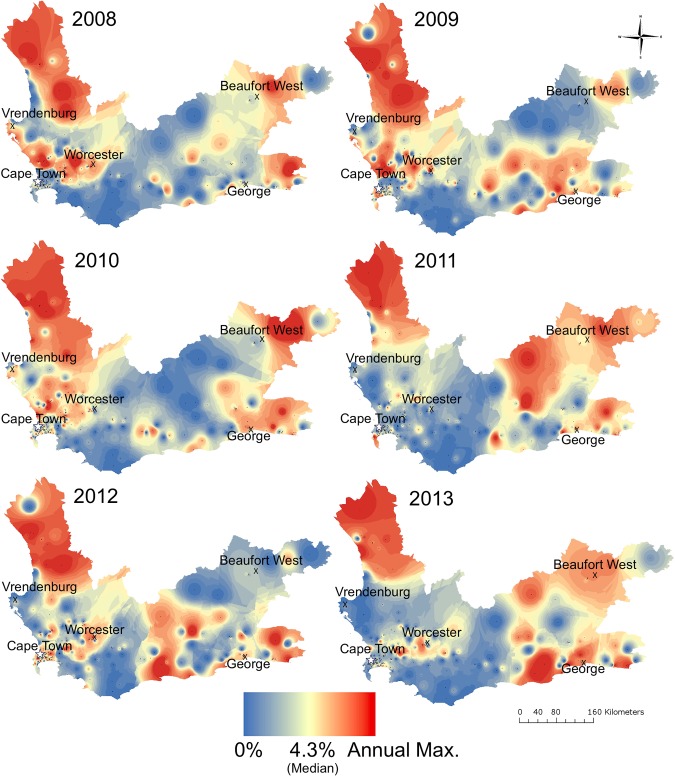
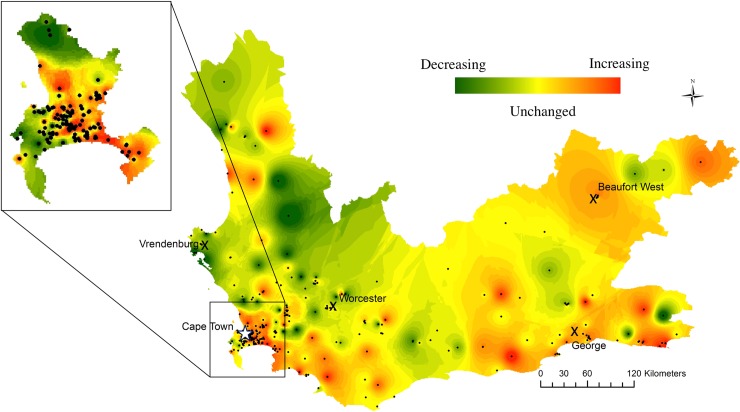
Methods and findings: We retrospectively identified cases of microbiologically confirmed tuberculosis and RR-tuberculosis from all biological samples submitted for tuberculosis testing (n = 2,219,891) to the Western Cape National Health Laboratory Services (NHLS) between January 1, 2008, and June 30, 2013. Because the NHLS database lacks unique patient identifiers, we performed a series of record-linking processes to match specimen records to individual patients. We counted an individual as having a single disease episode if their positive samples came from within two years of each other. Cases were aggregated by clinic location (n = 302) to estimate the percentage of tuberculosis cases with rifampicin resistance per clinic. We used inverse distance weighting (IDW) to produce heatmaps of the RR-tuberculosis percentage across the province. Regression was used to estimate annual changes in the RR-tuberculosis percentage by clinic, and estimated average size and direction of change was mapped. We identified 799,779 individuals who had specimens submitted from mappable clinics for testing, of whom 222,735 (27.8%) had microbiologically confirmed tuberculosis. The study population was 43% female, the median age was 36 years (IQR 27-44), and 10,255 (4.6%, 95% CI: 4.6-4.7) cases had documented rifampicin resistance. Among individuals with microbiologically confirmed tuberculosis, 8,947 (4.0%) had more than one disease episode during the study period. The percentage of tuberculosis cases with rifampicin resistance documented among these individuals was 11.4% (95% CI: 10.7-12.0). Overall, the percentage of tuberculosis cases that were RR-tuberculosis was spatially heterogeneous, ranging from 0% to 25% across the province. Our maps reveal significant yearly fluctuations in RR-tuberculosis percentages at several locations. Additionally, the directions of change over time in RR-tuberculosis percentage were not uniform. The main limitation of this study is the lack of unique patient identifiers in the NHLS database, rendering findings to be estimates reliant on the accuracy of the person-matching algorithm.
Conclusions: Our maps reveal striking spatial and temporal heterogeneity in RR-tuberculosis percentages across this province. We demonstrate the potential to monitor RR-tuberculosis spatially and temporally with routinely collected laboratory data, enabling improved resource targeting and more rapid locally appropriate interventions.
Conflict of interest statement
MBM is a member of the Editorial Board of PLOS Medicine. The authors declare no other competing interests exist.
Figures
References
-
- World Health Organization. Global tuberculosis report 2017. Geneva; 2017.
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
