

A retrospective case series of segmental zoster paresis of limbs: clinical, electrophysiological and imaging characteristics
- PMID: 30131076
- PMCID: PMC6102897
- DOI: 10.1186/s12883-018-1130-4
A retrospective case series of segmental zoster paresis of limbs: clinical, electrophysiological and imaging characteristics
Abstract
Background: Segmental zoster paresis (SZP) of limbs, characterized by focal weakness of extremity, is recognized as a rare complication of herpes zoster (HZ). The following study analyzes the clinical characteristics and data from electromyography and MRI scans in patients with motor weakness after zoster infection.
Methods: One thousand three hundred ninety-three patients from our database (Shandong Provincial Qianfoshan Hospital) suffering from HZ were retrospectively reviewed from June 2015 to July 2017. Patients who fulfilled the diagnostic criteria for SZP were included in the analysis. The clinical characteristics, as well as electromyography findings and MRI scans were analyzed.
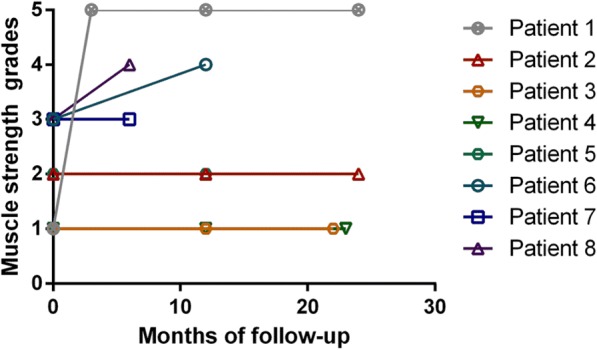
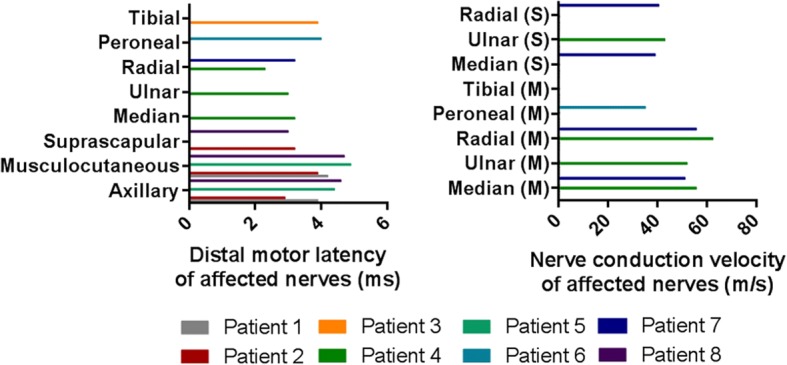
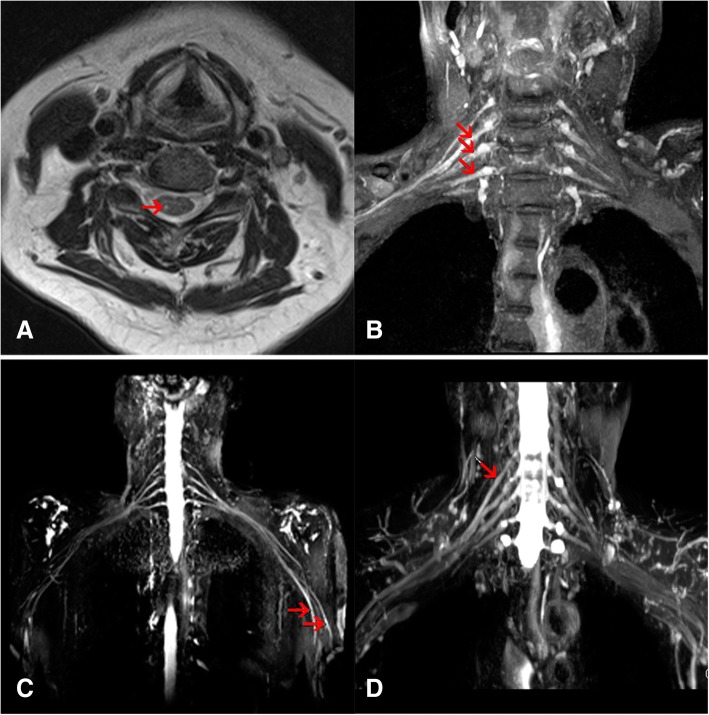
Results: SZP was present in 0.57% of patients with HZ (8/1393). The average age of symptom onset in 8 SZP patients was 69 years old (SD: 13, range 47-87). The severity of muscle weakness ranged from mild to severe. The electrophysiological testing revealed the characteristics of axonopathy. Radiculopathy (2/8), plexopathy (2/8), radiculoplexopathy (3/8) and combined radiculopathy and mononeuropathy (1/8) were also identified. MRI revealed hyperintensity of the affected spinal dorsal horns, nerve roots or peripheral nerves.
Conclusions: SZP is associated with obvious limb weakness, nerve axons lesions and localization to nerve roots, plexus or peripheral nerves.
Keywords: Electromyography; Herpes zoster; Infectious neuropathy; Nerve MRI; Nerve conduction; Segmental zoster paresis.
Conflict of interest statement
Ethics approval and consent to participate
This study was approved by the ethic committee of the Shandong Provincial Qianfoshan Hospital, Shandong University. Six patients signed the informed consents and two patients were not contacted before the submission. Exception to the requirement of informed consent was obtained from the ethic committee due to the retrospective study.
Consent for publication
Written informed consent was obtained from the patients described in cases (case 1, 2, 3, 5, 7and 8) for the publication of their personal and medical information and any accompanying images. A copy of the written consent is available for review by the Editor of this journal.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures

References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
