

First-in-Human Phase I Trial of a Tumor-Targeted Cytokine (NHS-IL12) in Subjects with Metastatic Solid Tumors
- PMID: 30131389
- PMCID: PMC6320276
- DOI: 10.1158/1078-0432.CCR-18-1512
First-in-Human Phase I Trial of a Tumor-Targeted Cytokine (NHS-IL12) in Subjects with Metastatic Solid Tumors
Abstract
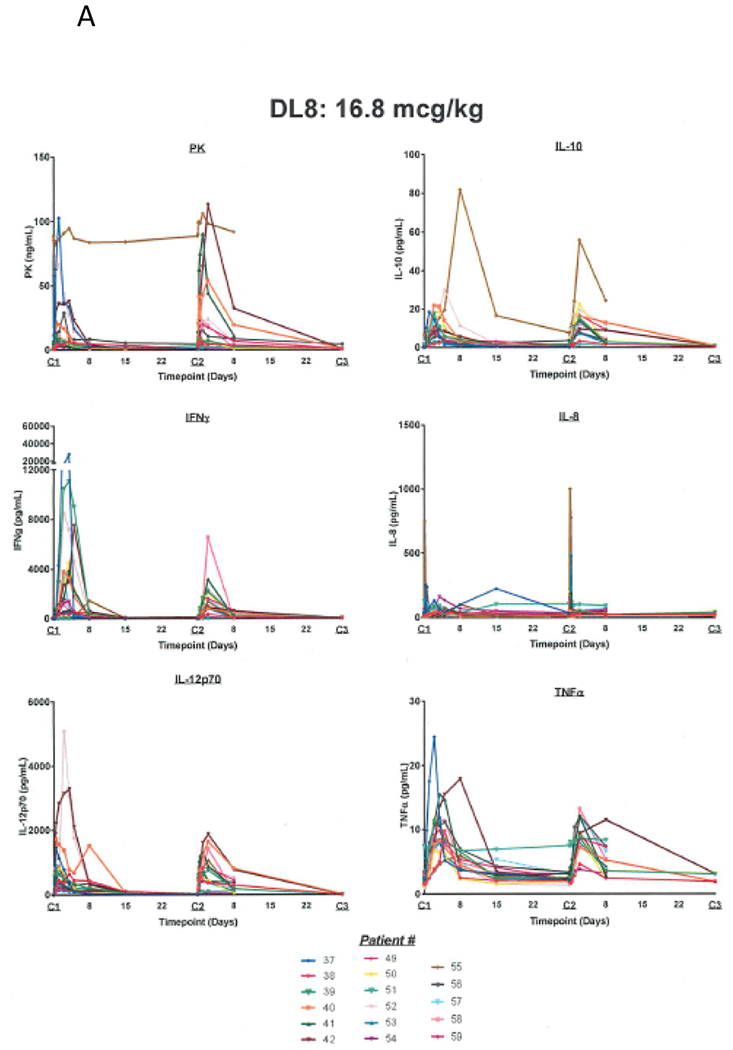
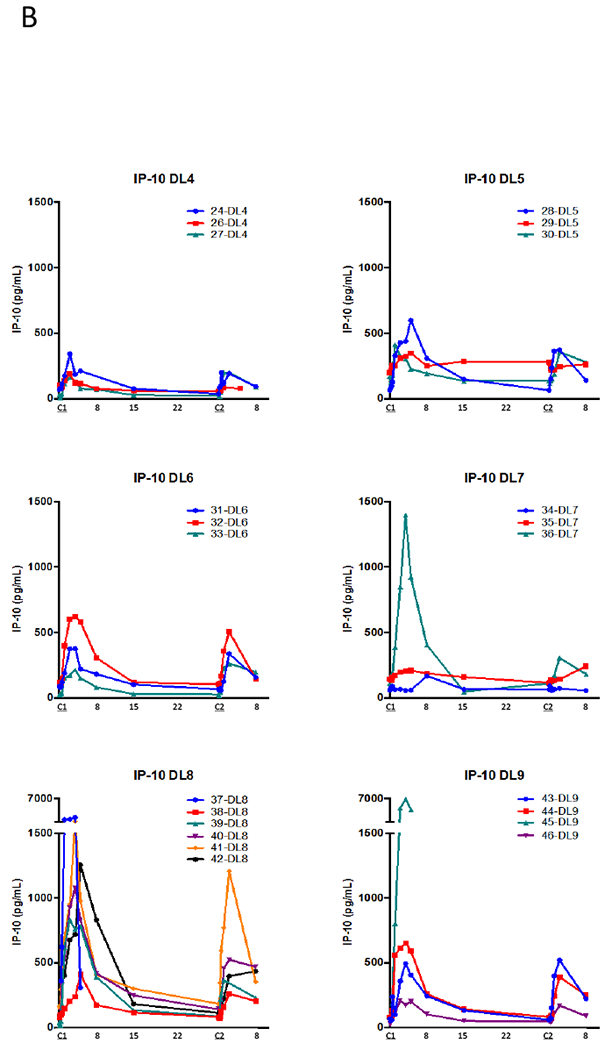
Purpose: The NHS-IL12 immunocytokine is composed of two IL12 heterodimers fused to the NHS76 antibody. Preclinical studies have shown that this antibody targets IL12 to regions of tumor necrosis by binding histones on free DNA fragments in these areas, resulting in enhanced antitumor activity. The objectives of this phase I study were to determine the maximum tolerated dose (MTD) and pharmacokinetics of NHS-IL12 in subjects with advanced solid tumors.
Patients and methods: Subjects (n = 59) were treated subcutaneously with NHS-IL12 in a single ascending-dose cohort followed by a multiple ascending-dose cohort (n = 37 with every 4-week dosing).
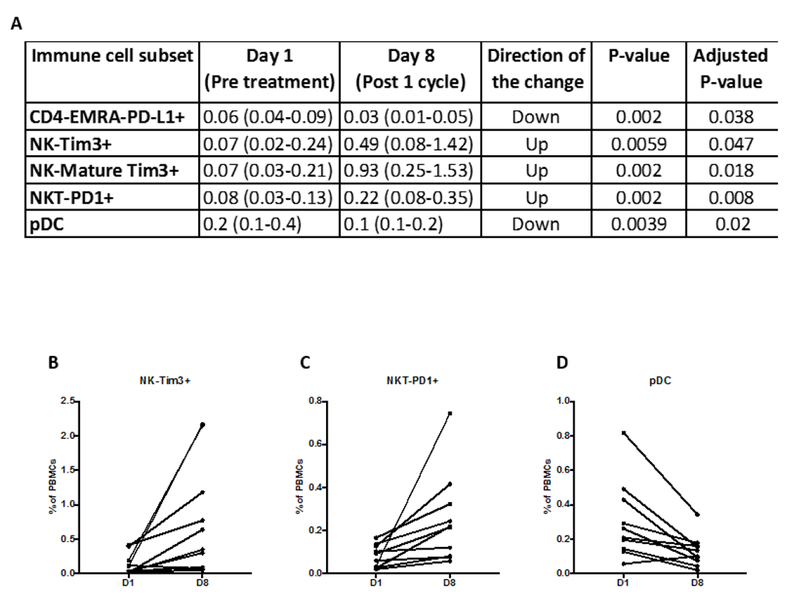
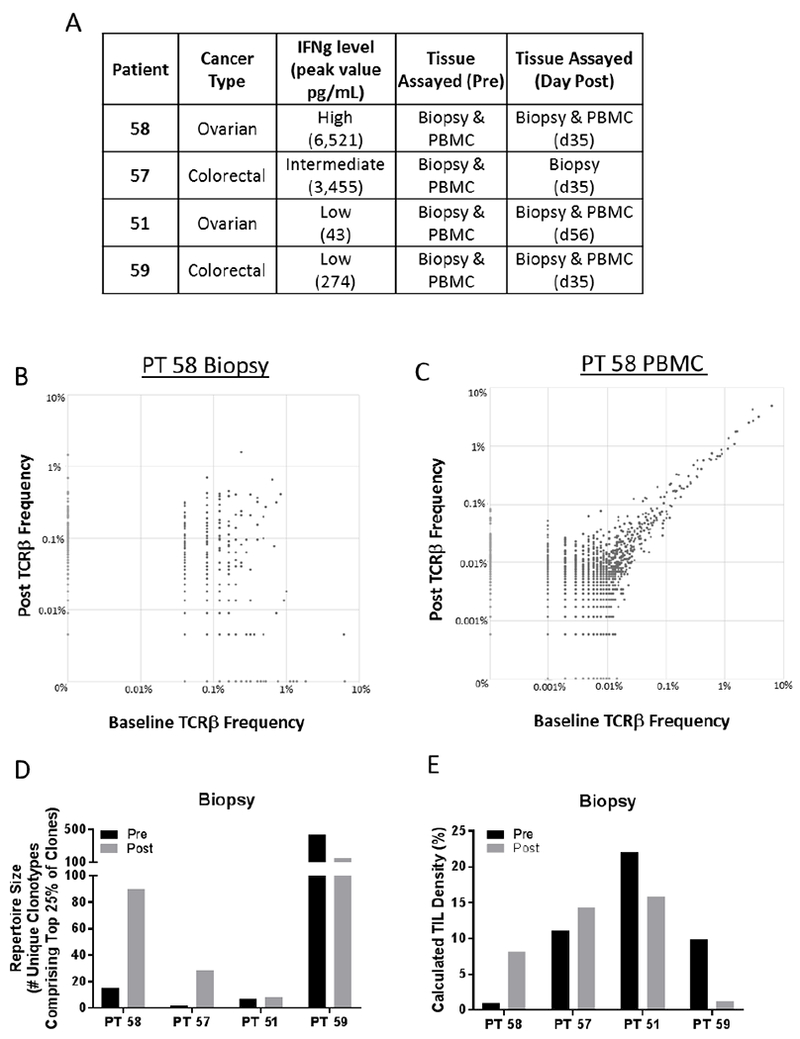
Results: The most frequently observed treatment-related adverse events (TRAE) included decreased circulating lymphocytes, increased liver transaminases, and flu-like symptoms. Of the grade ≥3 TRAEs, all were transient and only one was symptomatic (hyperhidrosis). The MTD is 16.8 μg/kg. A time-dependent rise in IFNγ and an associated rise in IL10 were observed following NHS-IL12. Of peripheral immune cell subsets evaluated, most noticeable were increases in frequencies of activated and mature natural killer (NK) cells and NKT cells. Based on T-cell receptor sequencing analysis, increases in T-cell receptor diversity and tumor-infiltrating lymphocyte density were observed after treatment where both biopsies and peripheral blood mononuclear cells were available. Although no objective tumor responses were observed, 5 subjects had durable stable disease (range, 6-30+ months).
Conclusions: NHS-IL12 was well tolerated up to a dose of 16.8 μg/kg, which is the recommended phase II dose. Early clinical immune-related activity warrants further studies, including combination with immune checkpoint inhibitors.See related commentary by Lyerly et al., p. 9.
©2018 American Association for Cancer Research.
Conflict of interest statement
Disclosure of Potential Conflicts of interest
C.R. Heery is an employee of Bavarian Nordic. No potential conflicts of interest were disclosed by the NIH authors.
Figures
Comment in
-
Right Time and Place for IL12: Targeted Delivery Stimulates Immune Therapy.Clin Cancer Res. 2019 Jan 1;25(1):9-11. doi: 10.1158/1078-0432.CCR-18-2819. Epub 2018 Oct 30. Clin Cancer Res. 2019. PMID: 30377197
References
-
- Aste-Amezaga M, D’Andrea A, Kubin M, Trinchieri G. Cooperation of natural killer cell stimulatory factor/interleukin-12 with other stimuli in the induction of cytokines and cytotoxic cell-associated molecules in human T and NK cells. Cell Immunol 1994;156:480–92. - PubMed
-
- van Herpen CM, van der Voort R, van der Laak JA, Klasen IS, de Graaf AO, van Kempen LC, et al. Intratumoral rhIL-12 administration in head and neck squamous cell carcinoma patients induces B cell activation. Int J Cancer 2008;123:2354–61. - PubMed
-
- Grohmann U, Belladonna ML, Bianchi R, Orabona C, Ayroldi E, Fioretti MC, et al. IL-12 acts directly on DC to promote nuclear localization of NF-kappaB and primes DC for IL-12 production. Immunity 1998;9:315–23. - PubMed
-
- Del Vecchio M, Bajetta E, Canova S, Lotze MT, Wesa A, Parmiani G, et al. Interleukin-12: biological properties and clinical application. Clin Cancer Res 2007;13:4677–85. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
