

PillCamColon2 after incomplete colonoscopy - A prospective multicenter study
- PMID: 30131662
- PMCID: PMC6102503
- DOI: 10.3748/wjg.v24.i31.3556
PillCamColon2 after incomplete colonoscopy - A prospective multicenter study
Abstract
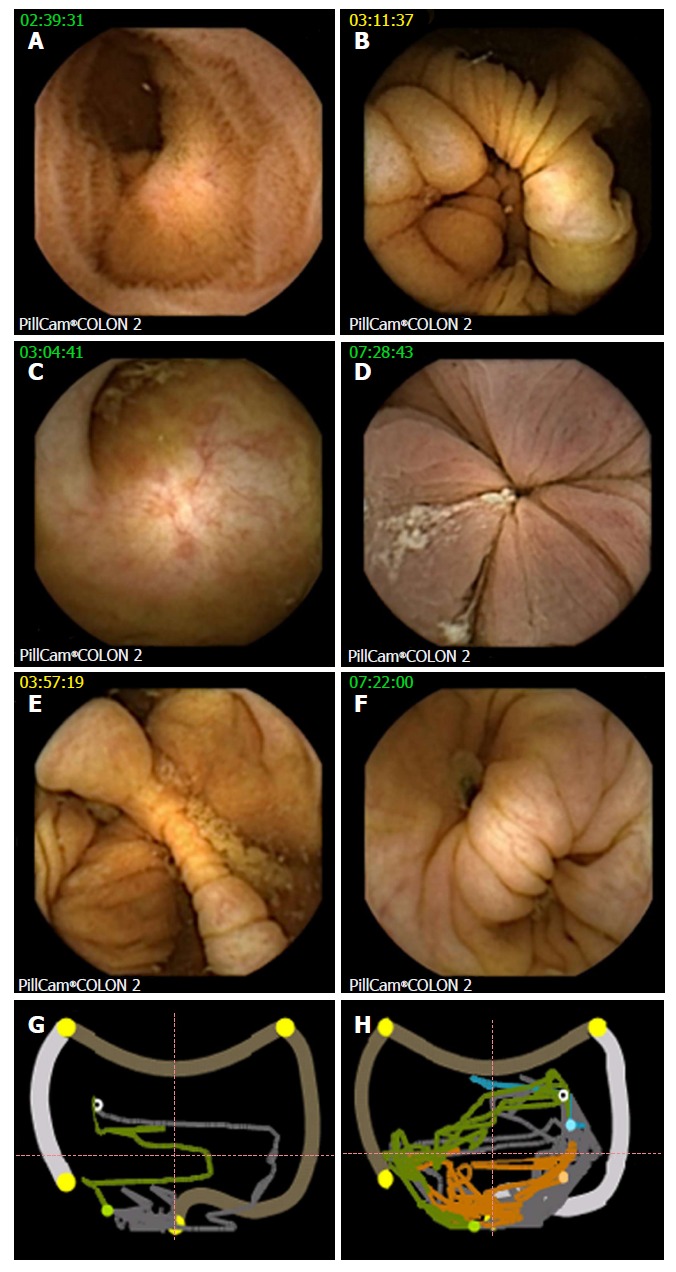
Aim: To evaluate the ability of PillCamColon2 to visualize colonic segments missed by incomplete optical colonoscopy (OC) and to assess the diagnostic yield.
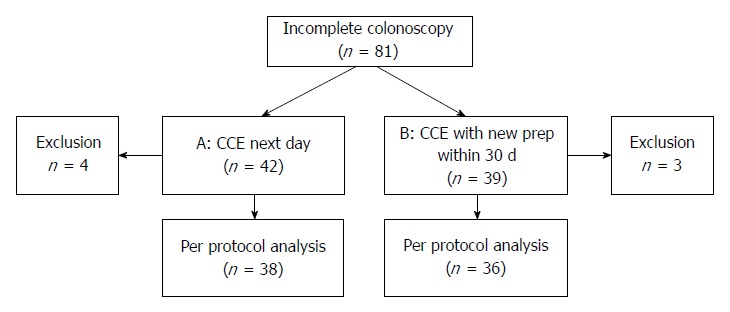
Methods: This prospective multicentre study included 81 patients from nine centres who underwent second-generation colon capsule endoscopy (CCE) following incomplete OC performed by an experienced gastroenterologist (> 1000 colonoscopies). Patients with stenosis were excluded. According to patient preferences, CCE was performed the following day (protocol A) after staying on clear liquids and 0.75 L Moviprep in the morning or within 30 d after new split-dose Moviprep (protocol B). Boosts consisted of 0.75 L and 0.25 L Moviprep, and phospho-soda was given as a rescue if the capsule was not excreted after seven hours.
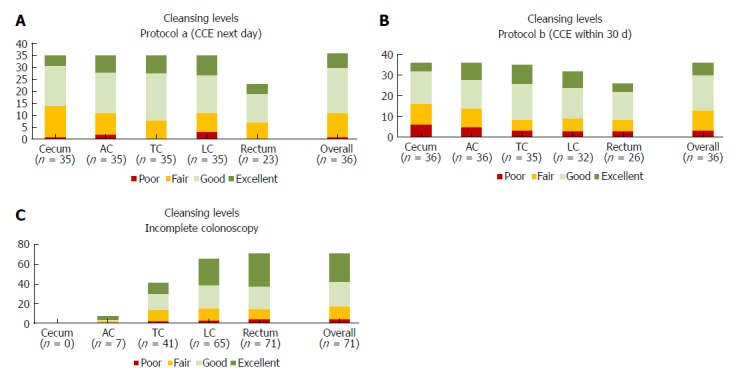
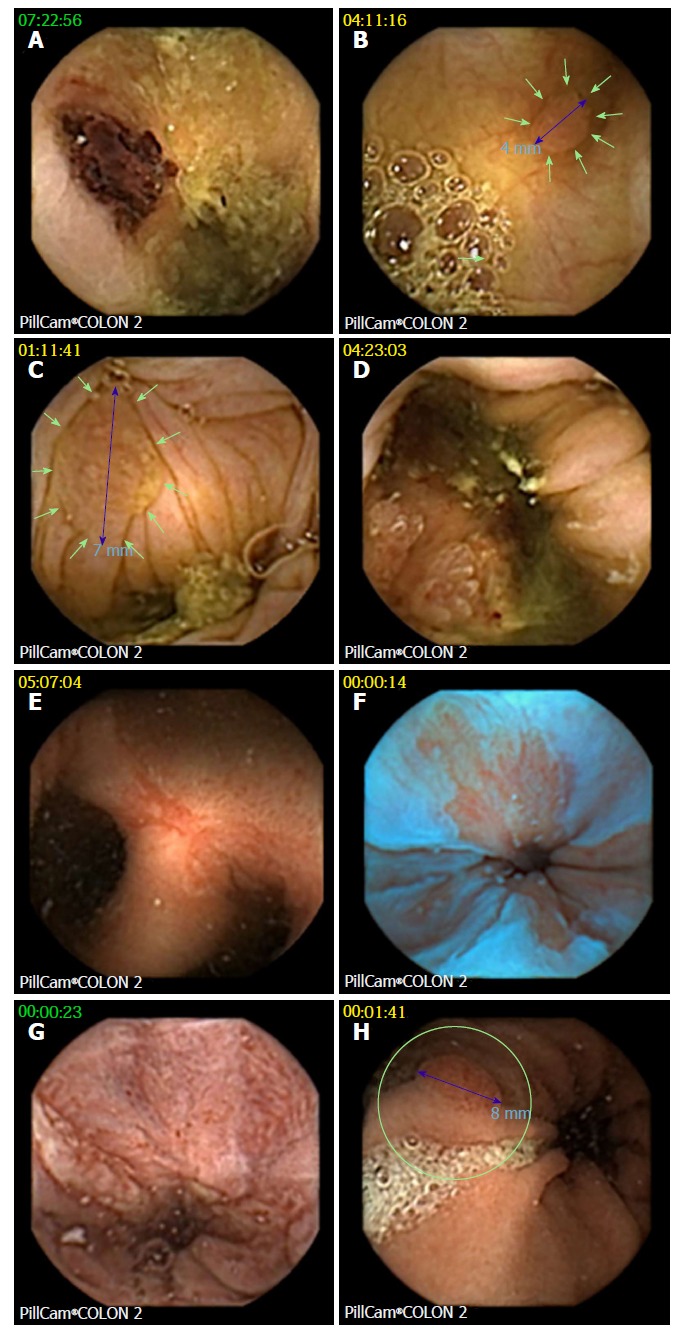
Results: Seventy-four patients were analysed (51% of them in group A; 49% in group B). Bowel cleansing was adequate in 67% of cases, and CCE could visualize colonic segments missed by incomplete colonoscopy in 90% of patients under protocol A and 97% of patients under protocol B (P = 0.35, n.s.). Significant polyps including adenocarcinoma were detected in 24% of cases. Detection rates for all polyps and significant polyps per patient were similar in both protocols. Polyps were found predominantly in the right colon (86%) in segments that were not reached by OC. Extracolonic findings - such as reflux esophagitis, suspected Barrett esophagus, upper GI-bleeding, gastric polyps, gastric erosions and angiectasia - were detected in eight patients. PillCamColon2 capsule was retained in the ileum of one patient (1.4%) without symptoms and removed during an uneventful resection for unknown Crohn's disease that was diagnosed as the cause of anemia, which was the indication for colonoscopy. CCE was well tolerated. One patient suffered from self-limiting vomiting after consuming the phospho-soda.
Conclusion: Second-generation CCE using a low-volume preparation is useful after incomplete OC, and it allows for the detection of additional relevant findings, but cleansing efficiency could be improved.
Keywords: Cleanliness level; Colon capsule endoscopy; Complementation rate; Incomplete colonoscopy; Low volume prep; Moviprep; Phospho-soda; PillCamColon2; Polyps.
Conflict of interest statement
Conflict-of-interest statement: Peter Baltes, Michael Philliper, Ingo Steinbrück, and Horst Hohn received lecture fees from Given Imaging, Jörg Albert, Martin Keuchel received study support and lecture fees from Given Imaging, Tanja Nowak was an employee of Given Imaging, the other authors have nothing to declare. The study was supported by Given Imaging, Hamburg, Germany by providing the capsules and an unrestricted grant.
Figures
References
-
- Pox CP, Altenhofen L, Brenner H, Theilmeier A, Von Stillfried D, Schmiegel W. Efficacy of a nationwide screening colonoscopy program for colorectal cancer. Gastroenterology. 2012;142:1460–1467.e2. - PubMed
-
- Brenner H, Altenhofen L, Katalinic A, Lansdorp-Vogelaar I, Hoffmeister M. Sojourn time of preclinical colorectal cancer by sex and age: estimates from the German national screening colonoscopy database. Am J Epidemiol. 2011;174:1140–1146. - PubMed
-
- Sarwar S, Anwar MM, Ryan B, O’Morain C. Colonoscopy completion rates - are we prepared for a national screening programme? Ir Med J. 2007;100:585–587. - PubMed
-
- Neerincx M, Terhaar sive Droste JS, Mulder CJ, Räkers M, Bartelsman JF, Loffeld RJ, Tuynman HA, Brohet RM, van der Hulst RW. Colonic work-up after incomplete colonoscopy: significant new findings during follow-up. Endoscopy. 2010;42:730–735. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
