

Surgical Standards for Management of the Axilla in Breast Cancer Clinical Trials with Pathological Complete Response Endpoint
- PMID: 30131975
- PMCID: PMC6098077
- DOI: 10.1038/s41523-018-0074-6
Surgical Standards for Management of the Axilla in Breast Cancer Clinical Trials with Pathological Complete Response Endpoint
Erratum in
-
Erratum: Author Correction: Surgical Standards for Management of the Axilla in Breast Cancer Clinical Trials with Pathological Complete Response Endpoint.NPJ Breast Cancer. 2019 Jan 2;5:2. doi: 10.1038/s41523-018-0096-0. eCollection 2019. NPJ Breast Cancer. 2019. PMID: 30675512 Free PMC article.
Abstract
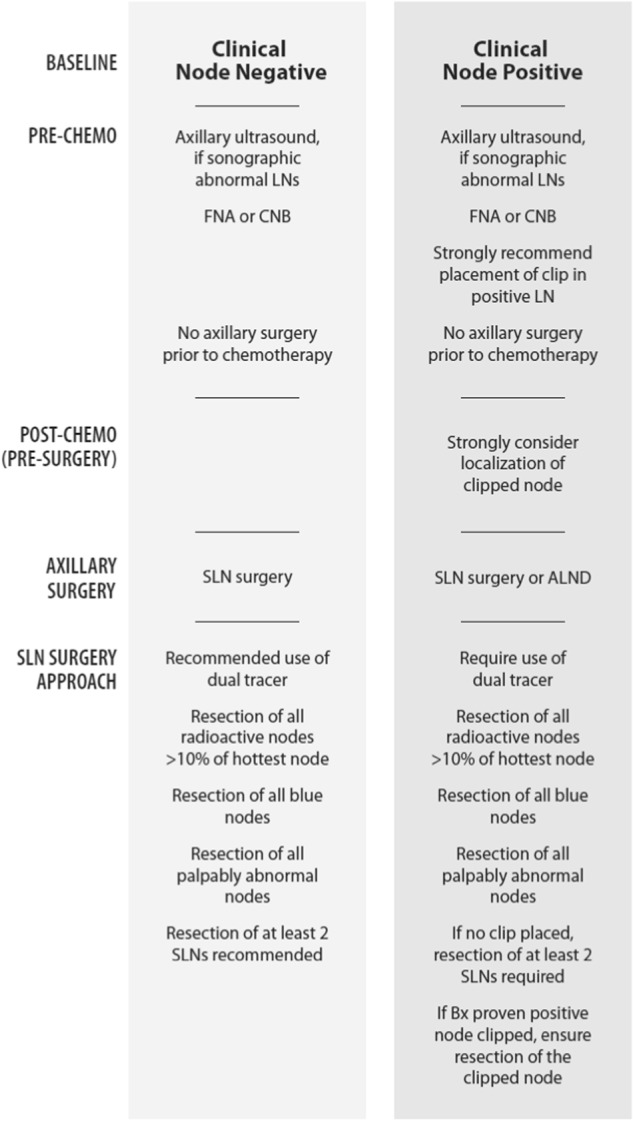
Advances in the surgical management of the axilla in patients treated with neoadjuvant chemotherapy, especially those with node positive disease at diagnosis, have led to changes in practice and more judicious use of axillary lymph node dissection that may minimize morbidity from surgery. However, there is still significant confusion about how to optimally manage the axilla, resulting in variation among practices. From the viewpoint of drug development, assessment of response to neoadjuvant chemotherapy remains paramount and appropriate assessment of residual disease-the primary endpoint of many drug therapy trials in the neoadjuvant setting-is critical. Therefore decreasing the variability, especially in a multicenter clinical trial setting, and establishing a minimum standard to ensure consistency in clinical trial data, without mandating axillary lymph node dissection, for all patients is necessary. The key elements which include proper staging and identification of nodal involvement at diagnosis, and appropriately targeted management of the axilla at the time of surgical resection are presented. The following protocols have been adopted as standard procedure by the I-SPY2 trial for management of axilla in patients with node positive disease, and present a framework for prospective clinical trials and practice.
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Krag DN, et al. Technical outcomes of sentinel-lymph-node resection and conventional axillary-lymph-node dissection in patients with clinically node-negative breast cancer: results from the NSABP B-32 randomised phase III trial. Lancet Oncol. 2007;8:881–888. doi: 10.1016/S1470-2045(07)70278-4. - DOI - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
