

Development of SGLT1 and SGLT2 inhibitors
- PMID: 30132033
- PMCID: PMC6124499
- DOI: 10.1007/s00125-018-4654-7
Development of SGLT1 and SGLT2 inhibitors
Abstract
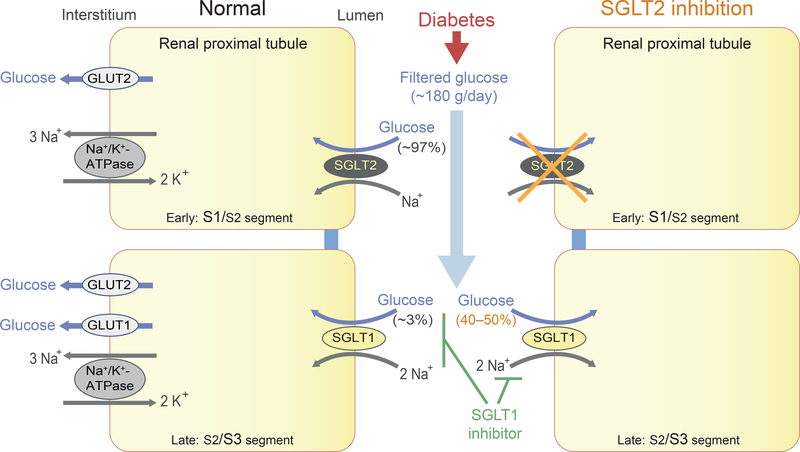
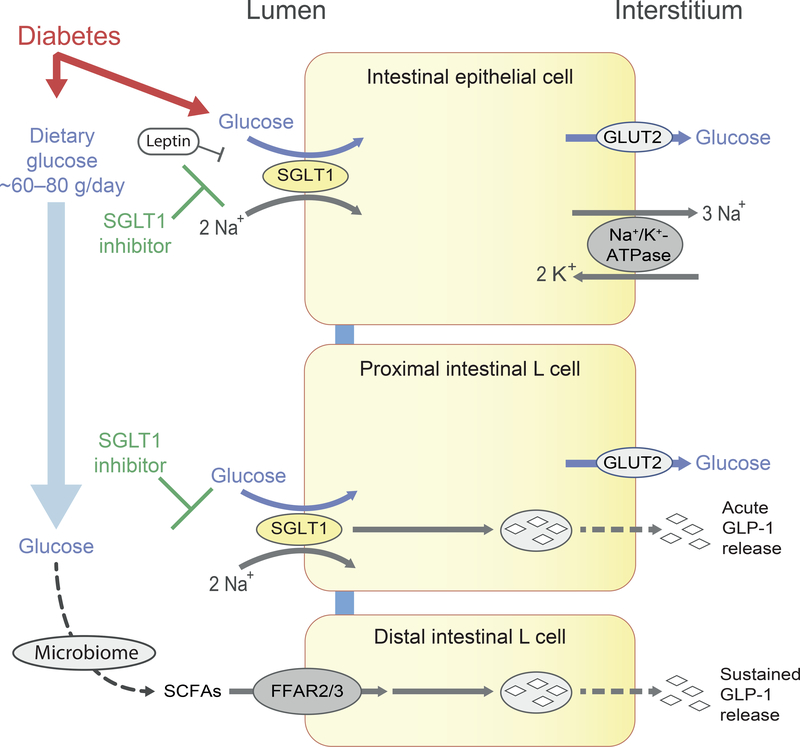
Sodium-glucose cotransporters SGLT1 (encoded by SGLT1, also known as SLC5A1) and SGLT2 (encoded by SGLT2, also known as SLC5A2) are important mediators of epithelial glucose transport. While SGLT1 accounts for most of the dietary glucose uptake in the intestine, SGLT2 is responsible for the majority of glucose reuptake in the tubular system of the kidney, with SGLT1 reabsorbing the remainder of the filtered glucose. As a consequence, mutations in the SLC5A1 gene cause glucose/galactose malabsorption, whereas mutations in SLC5A2 are associated with glucosuria. Since the cloning of SGLT1 more than 30 years ago, big strides have been made in our understanding of these transporters and their suitability as drug targets. Phlorizin, a naturally occurring competitive inhibitor of SGLT1 and SGLT2, provided the first insights into potential efficacy, but its use was hampered by intestinal side effects and a short half-life. Nevertheless, it was a starting point for the development of specific inhibitors of SGLT1 and SGLT2, as well as dual SGLT1/2 inhibitors. Since the approval of the first SGLT2 inhibitor in 2013 by the US Food and Drug Administration, SGLT2 inhibitors have become a new mainstay in the treatment of type 2 diabetes mellitus. They also have beneficial effects on the cardiovascular system (including heart failure) and the kidney. This review focuses on the rationale for the development of individual SGLT2 and SGLT1 inhibitors, as well as dual SGLT1/2 inhibition, including, but not limited to, aspects of genetics, genetically modified mouse models, mathematical modelling and general considerations of drug discovery in the field of metabolism.
Keywords: Chronic kidney disease; Drug development; Heart failure; Inhibitor; Intestinal glucose transport; Renal glucose transport; Review; Sodium–glucose cotransporter; Type 1 diabetes; Type 2 diabetes.
Figures
References
-
- Dennis VW, Brazy PC (1978) Phosphate and glucose transport in the proximal convoluted tubule: mutual dependency on sodium. Adv Exp Med Biol 103: 79–80 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
