

The motor repertoire of older adult fallers may constrain their response to balance perturbations
- PMID: 30133380
- PMCID: PMC6295530
- DOI: 10.1152/jn.00302.2018
The motor repertoire of older adult fallers may constrain their response to balance perturbations
Abstract
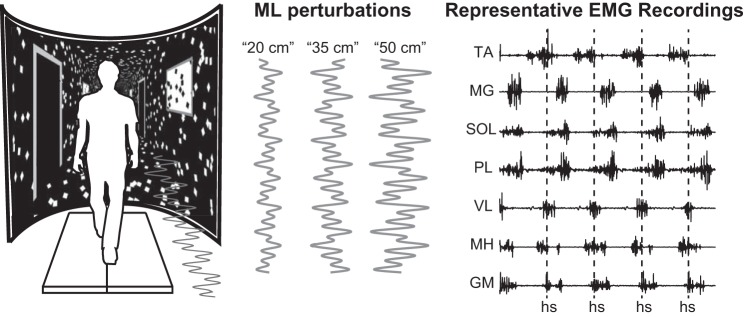
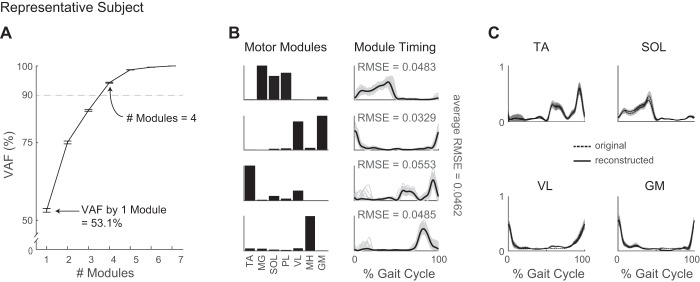
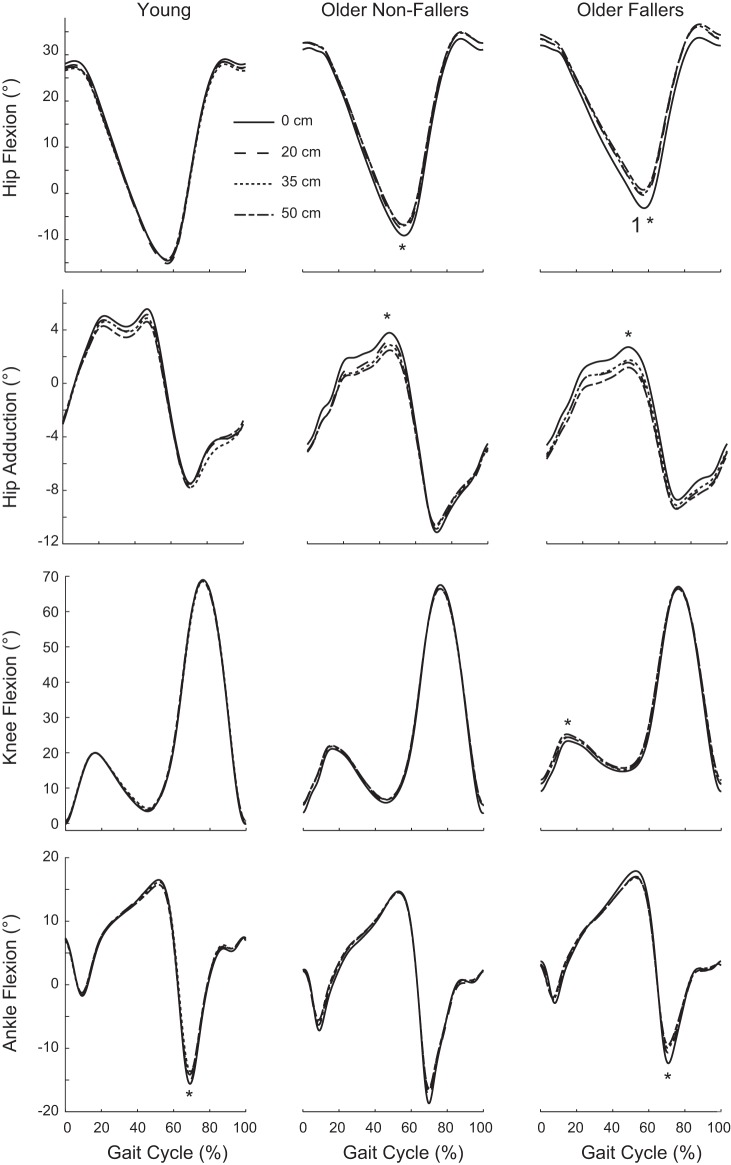
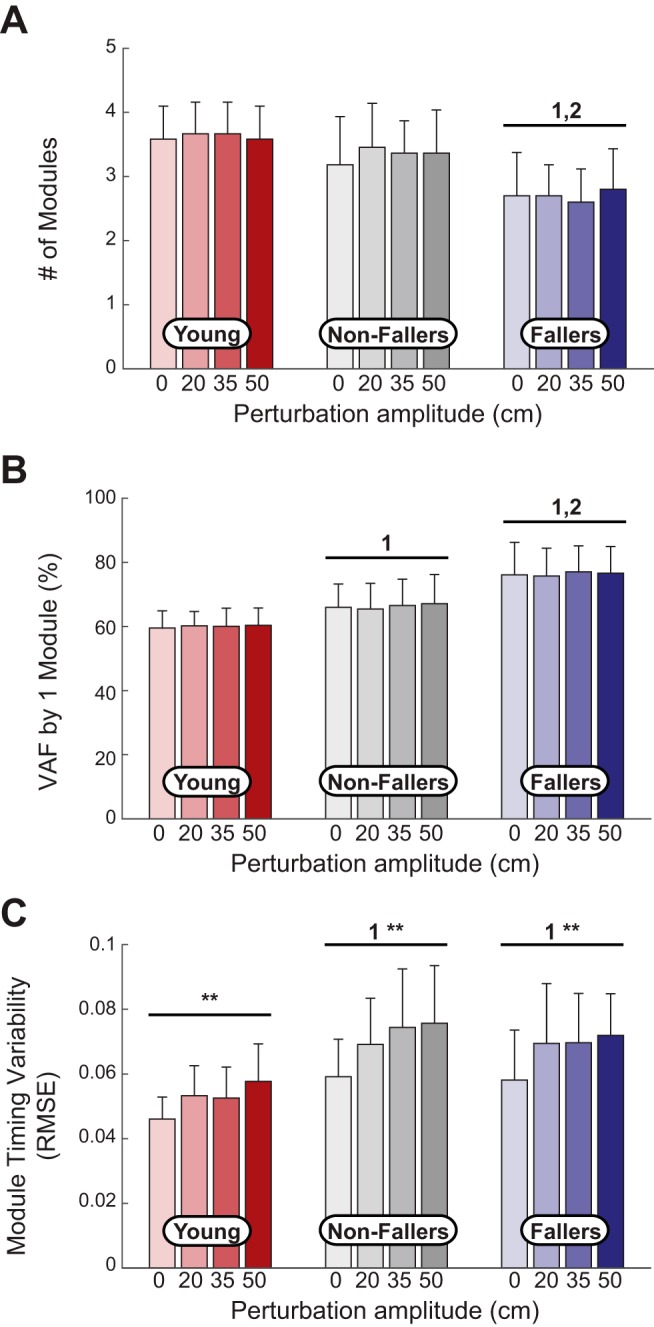
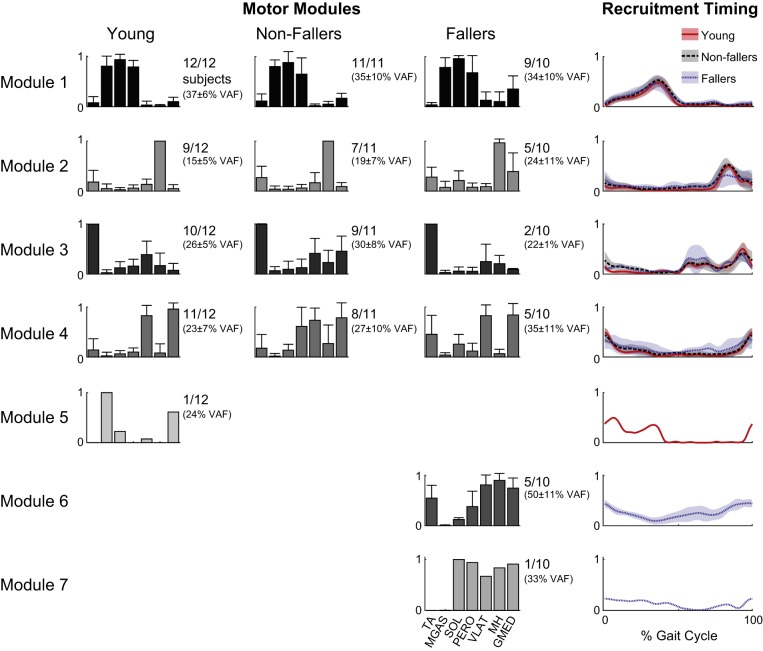
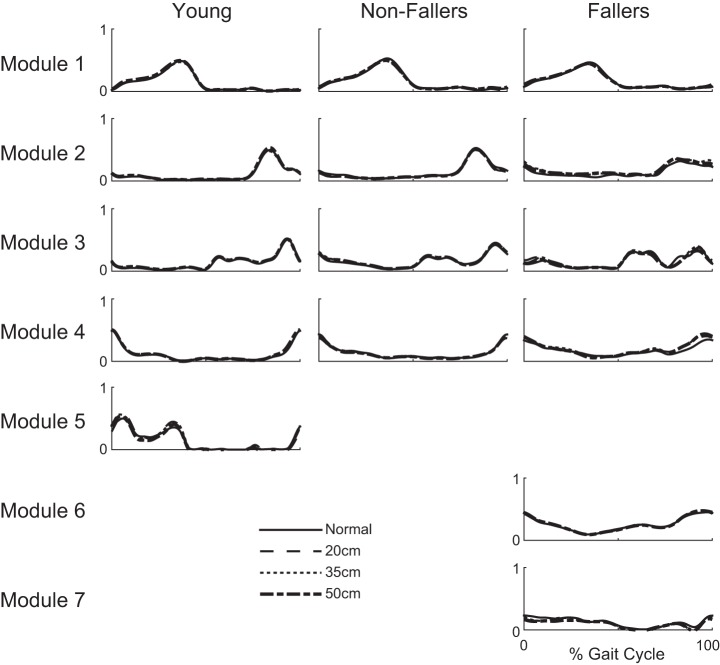
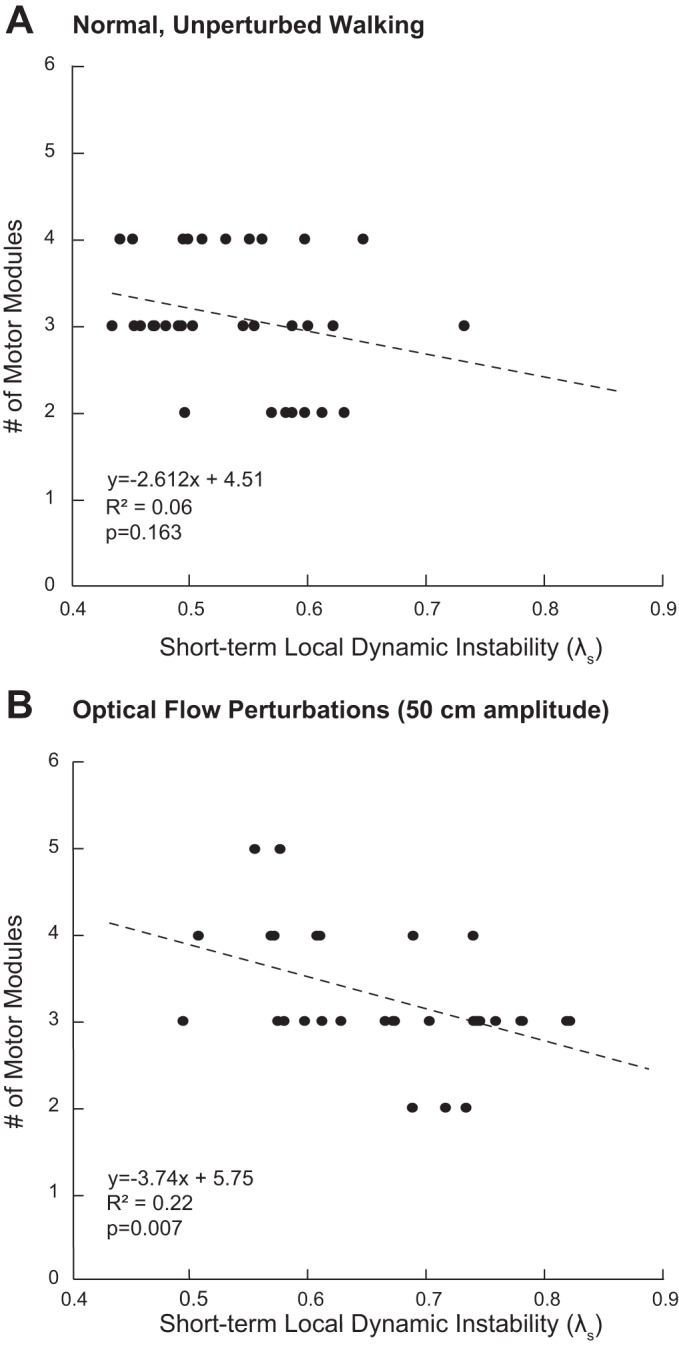
Older adults are at a high risk of falls, and most falls occur during locomotor activities like walking. This study aimed to improve our understanding of changes in neuromuscular control associated with increased risk of falls in older adults in the presence of dynamic balance challenges during walking. Motor module (also known as muscle synergy) analyses identified changes in the neuromuscular recruitment of leg muscles during walking with and without perturbations designed to elicit the visual perception of lateral instability. During normal walking we found that a history of falls (but not age) was associated with reduced motor module complexity and that age (but not a history of falls) was associated with increased step-to-step variability of module recruitment timing. Furthermore, motor module complexity was unaltered in the presence of optical flow perturbations. The specific effects of a history of falls on leg muscle recruitment included an absence and/or inability to independently recruit motor modules normally recruited to perform biomechanical functions important for walking balance control. These results suggest that fallers do not recruit the appropriate motor modules necessary for well-coordinated walking balance control even in the presence of perturbations. The identified changes in the modular control of walking balance in older fallers may either represent a neural deficit that leads to poor balance control or a prior history of falls that results in a compensatory motor adaptation. In either case, our study provides initial evidence that a reduced motor repertoire in older adult fallers may be a constraint on their ability to appropriately respond to balance challenges during walking. NEW & NOTEWORTHY This is the first study to demonstrate a reduced motor repertoire during walking in older adults with a history of falls but without any overt neurological deficits. Furthermore, using virtual reality during walking to elicit the visual perception of lateral instability, we provide initial evidence that a reduced motor repertoire in older adult fallers may be a constraint on their ability to appropriately respond to balance challenges during walking.
Keywords: gait; muscle synergy; stability; virtual reality; vision.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical