

Patient-specific anatomical model for deep brain stimulation based on 7 Tesla MRI
- PMID: 30133472
- PMCID: PMC6104927
- DOI: 10.1371/journal.pone.0201469
Patient-specific anatomical model for deep brain stimulation based on 7 Tesla MRI
Abstract
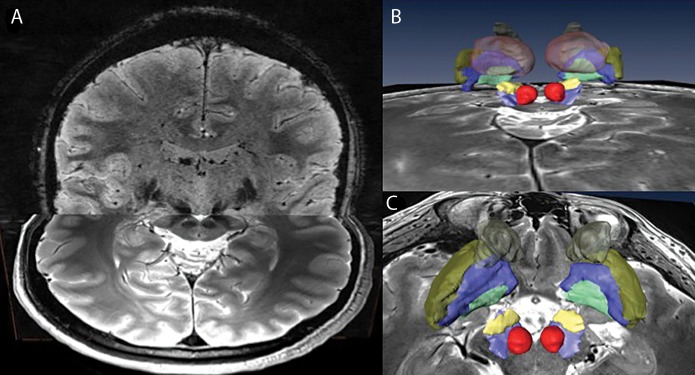
Objective: Deep brain stimulation (DBS) requires accurate localization of the anatomical target structure, and the precise placement of the DBS electrode within it. Ultra-high field 7 Tesla (T) MR images can be utilized to create patient-specific anatomical 3D models of the subthalamic nuclei (STN) to enhance pre-surgical DBS targeting as well as post-surgical visualization of the DBS lead position and orientation. We validated the accuracy of the 7T imaging-based patient-specific model of the STN and measured the variability of the location and dimensions across movement disorder patients.
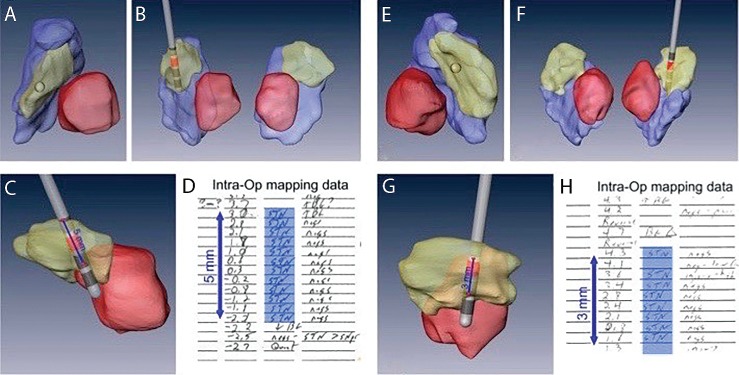
Methods: 72 patients who underwent DBS surgery were scanned preoperatively on 7T MRI. Segmentations and 3D volume rendering of the STN were generated for all patients. For 21 STN-DBS cases, microelectrode recording (MER) was used to validate the segmentation. For 12 cases, we computed the correlation between the overlap of the STN and volume of tissue activated (VTA) and the monopolar review for a further validation of the model's accuracy and its clinical relevancy.
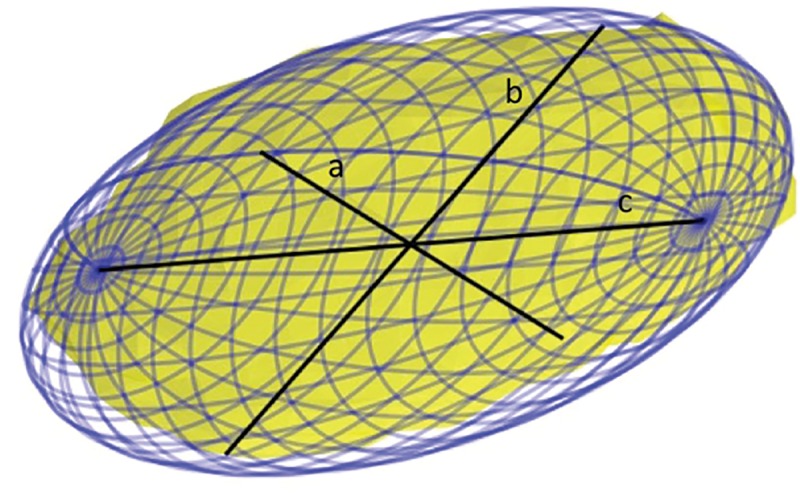
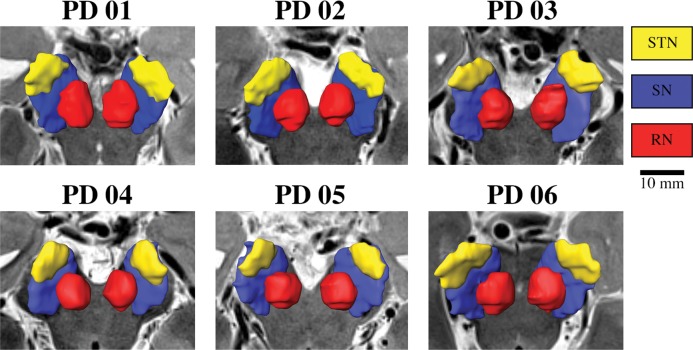
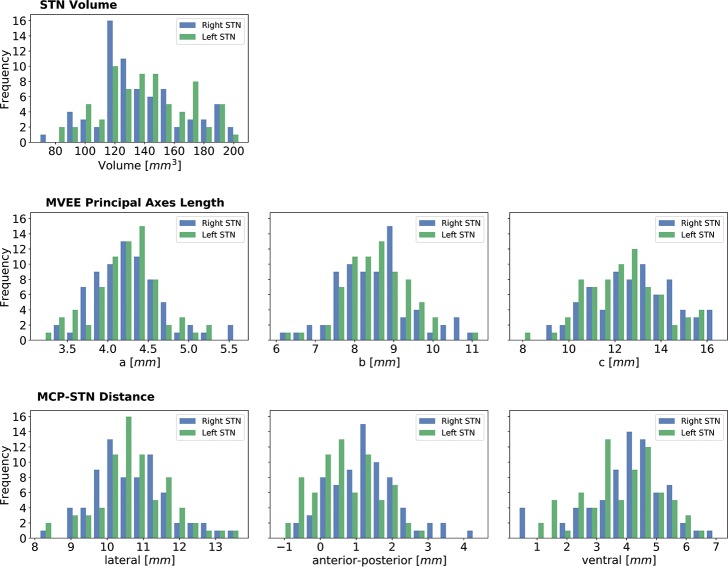
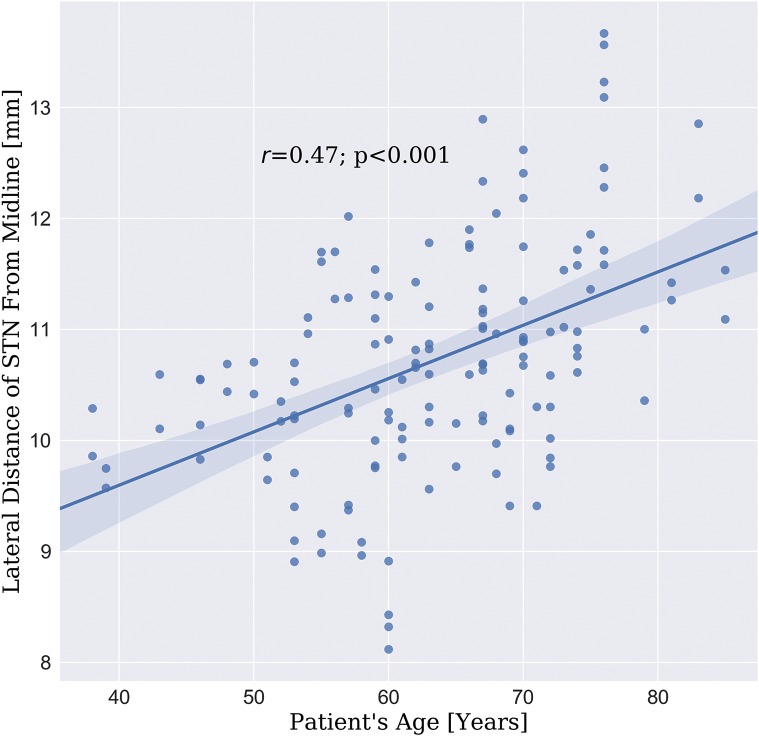
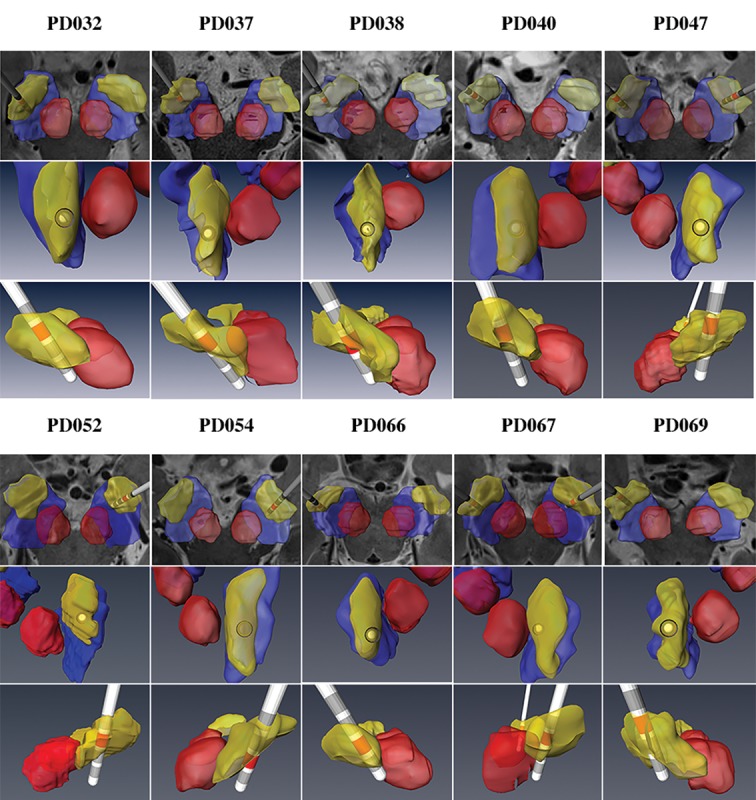
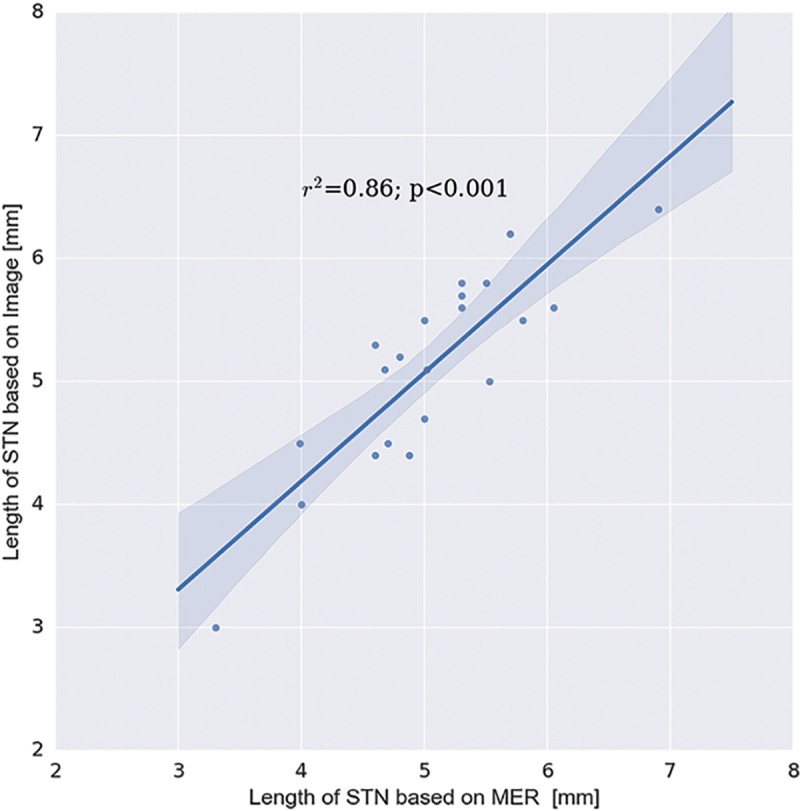
Results: We successfully reconstructed and visualized the STN in all patients. Significant variability was found across individuals regarding the location of the STN center of mass as well as its volume, length, depth and width. Significant correlations were found between MER and the 7T imaging-based model of the STN (r = 0.86) and VTA-STN overlap and the monopolar review outcome (r = 0.61).
Conclusion: The results suggest that an accurate visualization and localization of a patient-specific 3D model of the STN can be generated based on 7T MRI. The imaging-based 7T MRI STN model was validated using MER and patient's clinical outcomes. The significant variability observed in the STN location and shape based on a large number of patients emphasizes the importance of an accurate direct visualization of the STN for DBS targeting. An accurate STN localization can facilitate postoperative stimulation parameters for optimized patient outcome.
Conflict of interest statement
Yuval Duchin, Reuben R Shamir and Jinyoung Kim are employees of Surgical Information Sciences. Remi Patriat, Jerrold L. Vitek, Guillermo Sapiro and Noam Harel are shareholders of Surgical Information Sciences. This does not alter our adherence to PLOS ONE policies on sharing data and materials.
Figures




References
-
- Yelnik J, Damier P, Demeret S, Gervais D, Bardinet E, Bejjani B-P, et al. Localization of stimulating electrodes in patients with Parkinson disease by using a three-dimensional atlas—magnetic resonance imaging coregistration method. J Neurosurg. 2003;99: 89–99. 10.3171/jns.2003.99.1.0089 - DOI - PubMed
-
- Pallavaram S, DʼHaese P-F, Lake W, Konrad PE, Dawant BM, Neimat JS. Fully automated targeting using nonrigid image registration matches accuracy and exceeds precision of best manual approaches to subthalamic deep brain stimulation targeting in Parkinson disease. Neurosurgery. NIH Public Access; 2015;76: 756–65. 10.1227/NEU.0000000000000714 - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
