

Non-alcoholic fatty liver disease is a strong predictor of coronary artery calcification in metabolically healthy subjects: A cross-sectional, population-based study in middle-aged subjects
- PMID: 30133541
- PMCID: PMC6105021
- DOI: 10.1371/journal.pone.0202666
Non-alcoholic fatty liver disease is a strong predictor of coronary artery calcification in metabolically healthy subjects: A cross-sectional, population-based study in middle-aged subjects
Abstract
Objectives: This study aims to estimate the relationship between non-alcoholic fatty liver disease (NAFLD) and measures of atherosclerotic cardiovascular disease (ASCVD), and to determine to what extent such relationships are modified by metabolic risk factors.
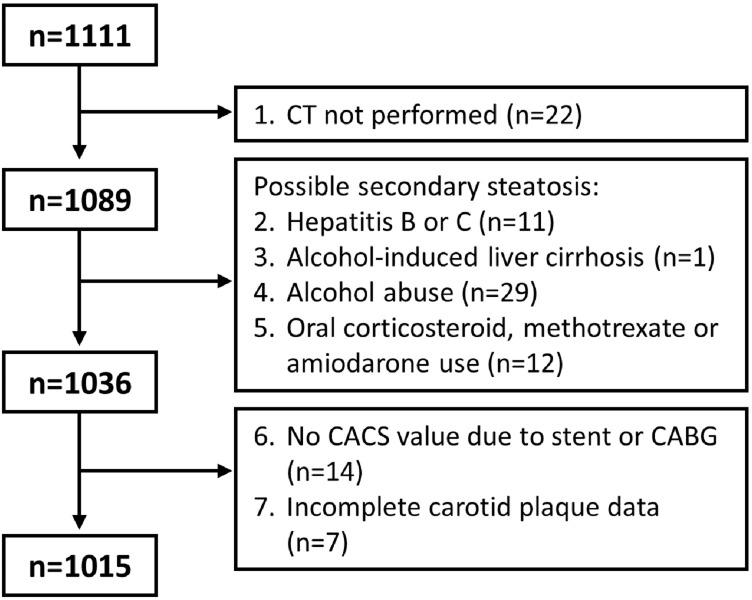
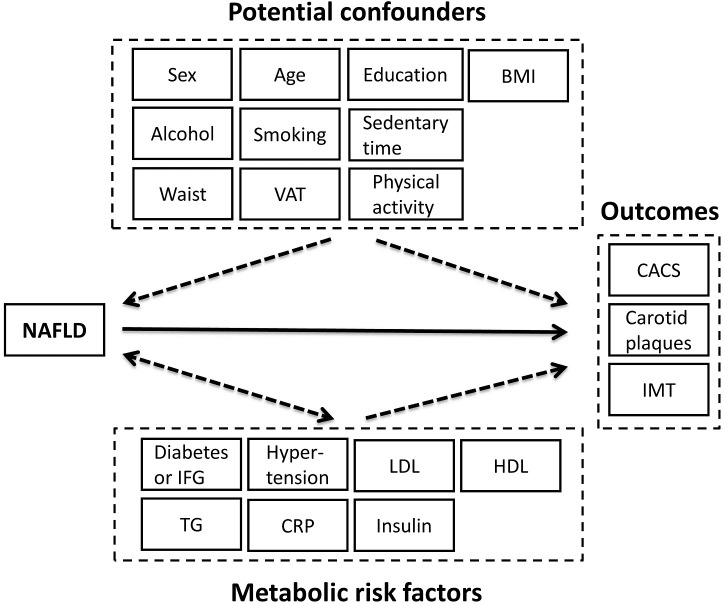
Methods: The study was conducted in the population-based Swedish CArdioPulmonary bioImage Study (SCAPIS) pilot cohort (n = 1015, age 50-64 years, 51.2% women). NAFLD was defined as computed tomography liver attenuation ≤40 Hounsfield Units, excluding other causes of liver fat. Coronary artery calcification score (CACS) was assessed using the Agatston method. Carotid plaques and intima media thickness (IMT) were measured by ultrasound. Metabolic status was based on assessments of glucose homeostasis, serum lipids, blood pressure and inflammation. A propensity score model was used to balance NAFLD and non NAFLD groups with regards to potential confounders and associations between NAFLD status and ASCVD variables in relation to metabolic status were examined by logistic and generalized linear regression models.
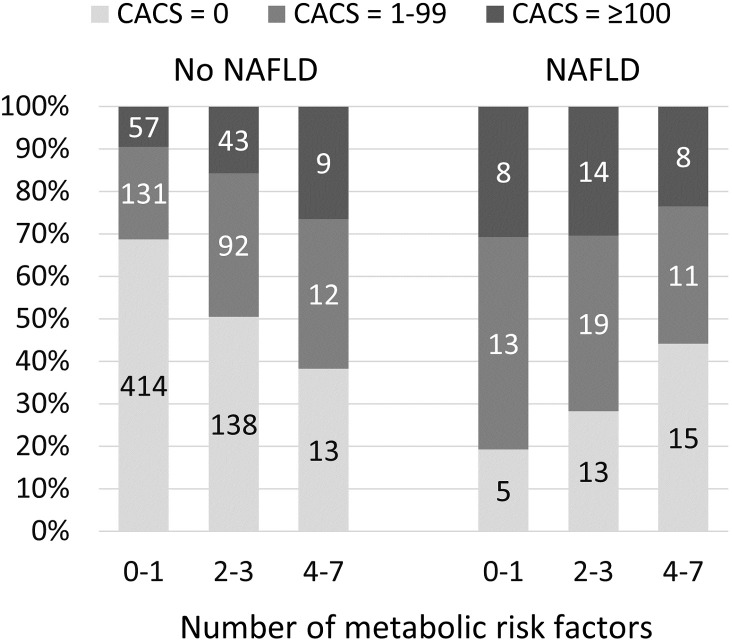
Results: NAFLD was present in 106 (10.4%) of the subjects and strongly associated with obesity-related traits. NAFLD was significantly associated with CACS after adjustment for confounders and metabolic risk factors (OR 1.77, 95% CI 1.07-2.94), but not with carotid plaques and IMT. The strongest association between NAFLD and CACS was observed in subjects with few metabolic risk factors (n = 612 [60% of all] subjects with 0-1 out of 7 predefined metabolic risk factors; OR 5.94, 95% CI 2.13-16.6).
Conclusions: NAFLD was independently associated with coronary artery calcification but not with measures of carotid atherosclerosis in this cohort. The association between NAFLD and CACS was most prominent in the metabolically healthy subjects.
Conflict of interest statement
J.K. is cofounder and employee of Antaros Medical, Sweden. S.L. has received fees from Intercept Pharmaceuticals for lecturing and advisory board participation. A.G. is a part time employee at Antaros Medical, Sweden. All other authors declared they do not have anything to disclose regarding conflict of interest with respect to this manuscript. This does not alter our adherence to PLOS ONE policies on sharing data and materials.
Figures
References
-
- Al Rifai M, Silverman MG, Nasir K, Budoff MJ, Blankstein R, Szklo M, et al. The association of nonalcoholic fatty liver disease, obesity, and metabolic syndrome, with systemic inflammation and subclinical atherosclerosis: the Multi-Ethnic Study of Atherosclerosis (MESA). Atherosclerosis. 2015;239(2):629–33. 10.1016/j.atherosclerosis.2015.02.011 ; PubMed Central PMCID: PMC4406399. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
