

Ultrasound Assessment of the Change in Carotid Corrected Flow Time in Fluid Responsiveness in Undifferentiated Shock
- PMID: 30134304
- PMCID: PMC6774608
- DOI: 10.1097/CCM.0000000000003356
Ultrasound Assessment of the Change in Carotid Corrected Flow Time in Fluid Responsiveness in Undifferentiated Shock
Abstract
Objectives: Adequate assessment of fluid responsiveness in shock necessitates correct interpretation of hemodynamic changes induced by preload challenge. This study evaluates the accuracy of point-of-care Doppler ultrasound assessment of the change in carotid corrected flow time induced by a passive leg raise maneuver as a predictor of fluid responsiveness. Noninvasive cardiac output monitoring (NICOM, Cheetah Medical, Newton Center, MA) system based on a bioreactance method was used.
Design: Prospective, noninterventional study.
Setting: ICU at a large academic center.
Patients: Patients with new, undifferentiated shock, and vasopressor requirements despite fluid resuscitation were included. Patients with significant cardiac disease and conditions that precluded adequate passive leg raising were excluded.
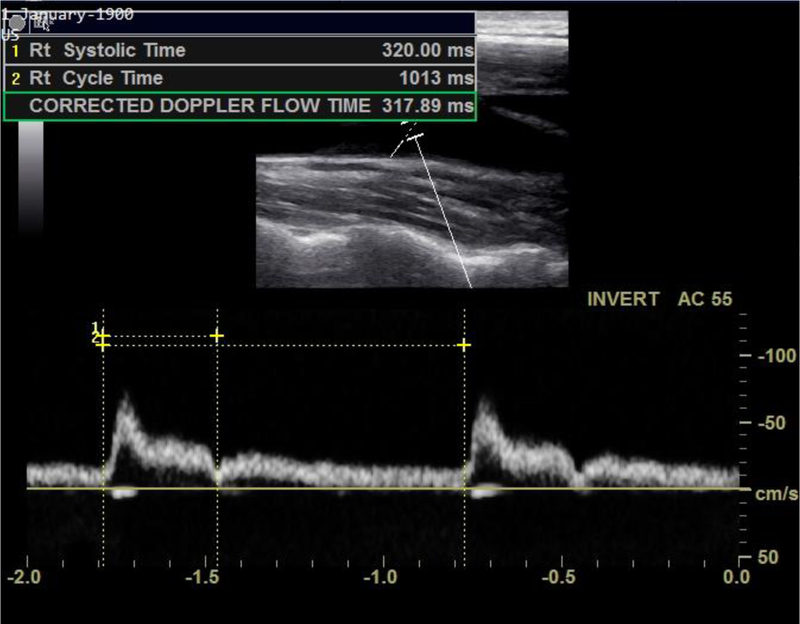
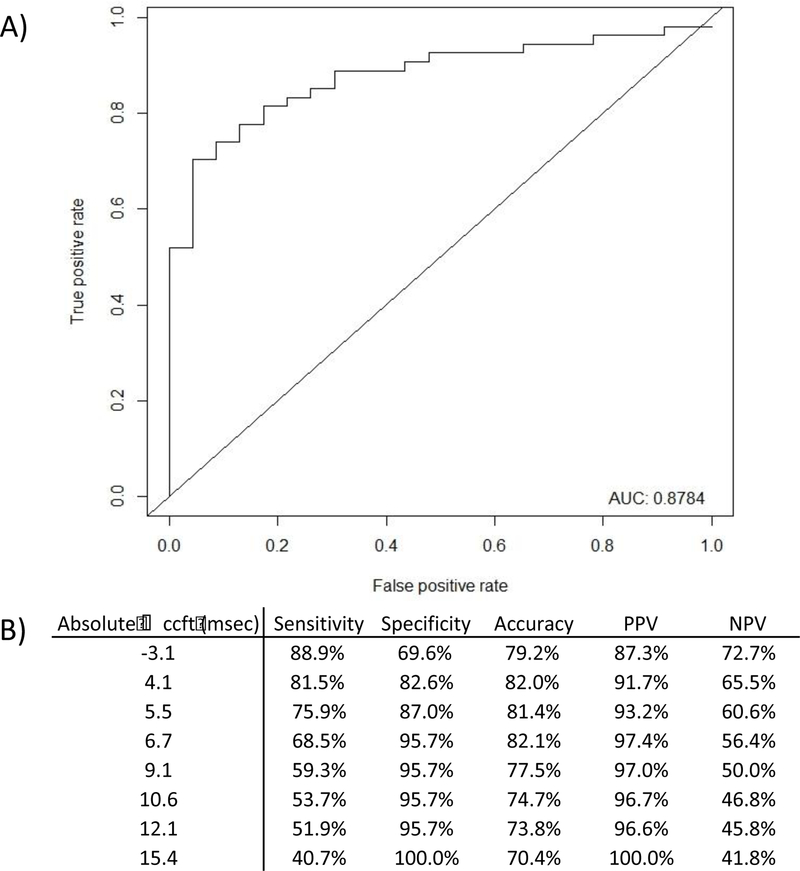
Interventions: Carotid corrected flow time was measured via ultrasound before and after a passive leg raise maneuver. Predicted fluid responsiveness was defined as greater than 10% increase in stroke volume on noninvasive cardiac output monitoring following passive leg raise. Images and measurements were reanalyzed by a second, blinded physician. The accuracy of change in carotid corrected flow time to predict fluid responsiveness was evaluated using receiver operating characteristic analysis.
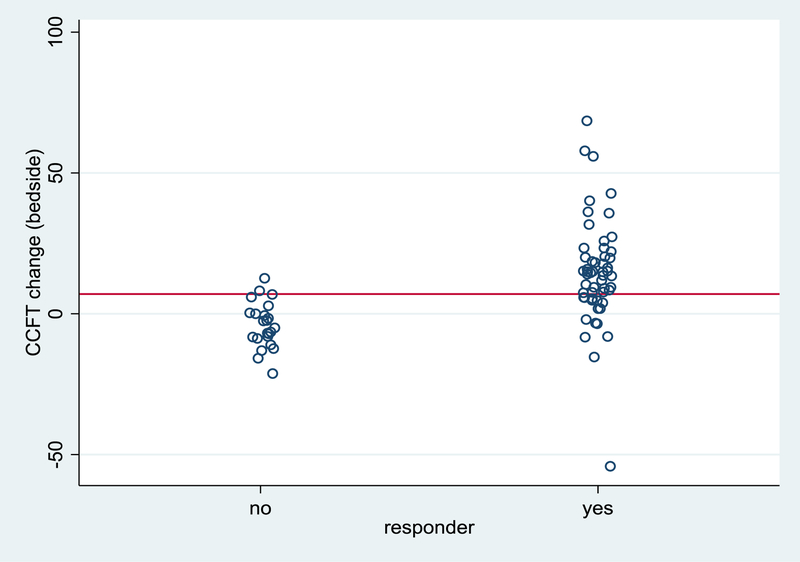
Measurements and main results: Seventy-seven subjects were enrolled with 54 (70.1%) classified as fluid responders by noninvasive cardiac output monitoring. The average change in carotid corrected flow time after passive leg raise for fluid responders was 14.1 ± 18.7 ms versus -4.0 ± 8 ms for nonresponders (p < 0.001). Receiver operating characteristic analysis demonstrated that change in carotid corrected flow time is an accurate predictor of fluid responsiveness status (area under the curve, 0.88; 95% CI, 0.80-0.96) and a 7 ms increase in carotid corrected flow time post passive leg raise was shown to have a 97% positive predictive value and 82% accuracy in detecting fluid responsiveness using noninvasive cardiac output monitoring as a reference standard. Mechanical ventilation, respiratory rate, and high positive end-expiratory pressure had no significant impact on test performance. Post hoc blinded evaluation of bedside acquired measurements demonstrated agreement between evaluators.
Conclusions: Change in carotid corrected flow time can predict fluid responsiveness status after a passive leg raise maneuver. Using point-of-care ultrasound to assess change in carotid corrected flow time is an acceptable and reproducible method for noninvasive identification of fluid responsiveness in critically ill patients with undifferentiated shock.
Conflict of interest statement
Conflicts of interest
The remaining authors have disclosed that they have no relevant financial conflicts of interest.
Figures
Similar articles
-
The use of bioreactance and carotid Doppler to determine volume responsiveness and blood flow redistribution following passive leg raising in hemodynamically unstable patients.Chest. 2013 Feb 1;143(2):364-370. doi: 10.1378/chest.12-1274. Chest. 2013. PMID: 22910834
-
Evaluation of the fluid responsiveness in patients with septic shock by ultrasound plus the passive leg raising test.J Surg Res. 2018 Apr;224:207-214. doi: 10.1016/j.jss.2017.12.014. Epub 2018 Jan 4. J Surg Res. 2018. PMID: 29506842
-
Accuracy assessment of noninvasive cardiac output monitoring in the hemodynamic monitoring in critically ill patients.Ann Palliat Med. 2020 Sep;9(5):3506-3512. doi: 10.21037/apm-20-1731. Ann Palliat Med. 2020. PMID: 33065801
-
Predicting fluid responsiveness: A review of literature and a guide for the clinician.Am J Emerg Med. 2018 Nov;36(11):2093-2102. doi: 10.1016/j.ajem.2018.08.037. Epub 2018 Aug 14. Am J Emerg Med. 2018. PMID: 30122506 Review.
-
Will This Hemodynamically Unstable Patient Respond to a Bolus of Intravenous Fluids?JAMA. 2016 Sep 27;316(12):1298-309. doi: 10.1001/jama.2016.12310. JAMA. 2016. PMID: 27673307 Review.
Cited by
-
The left ventricular outflow tract and carotid artery velocity time integrals.Front Med Technol. 2024 Jan 24;6:1320810. doi: 10.3389/fmedt.2024.1320810. eCollection 2024. Front Med Technol. 2024. PMID: 38333734 Free PMC article.
-
Changes in the corrected carotid flow time can predict spinal anesthesia-induced hypotension in patients undergoing cesarean delivery: an observational study.J Anesth. 2024 Feb;38(1):105-113. doi: 10.1007/s00540-023-03293-2. Epub 2024 Jan 3. J Anesth. 2024. PMID: 38172292
-
Evaluation of hemorrhagic shock and fluid resuscitation in pigs using handless Doppler carotid artery ultrasound.Eur J Trauma Emerg Surg. 2024 Aug;50(4):1513-1520. doi: 10.1007/s00068-024-02481-3. Epub 2024 Mar 1. Eur J Trauma Emerg Surg. 2024. PMID: 38427062 Free PMC article.
-
A Carotid Doppler Patch Accurately Tracks Stroke Volume Changes During a Preload-Modifying Maneuver in Healthy Volunteers.Crit Care Explor. 2020 Jan 29;2(1):e0072. doi: 10.1097/CCE.0000000000000072. eCollection 2020 Jan. Crit Care Explor. 2020. PMID: 32166292 Free PMC article.
-
A framework for flow time measured by Doppler ultrasound.Ultrasound J. 2025 Jan 21;17(1):10. doi: 10.1186/s13089-025-00414-8. Ultrasound J. 2025. PMID: 39836314 Free PMC article.
References
-
- Rhodes A, Evans LE, Alhazzani W, et al.: Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016. Intensive Care Med 2017, 43(3):304–377. - PubMed
-
- Rupp SM, Apfelbaum JL, Blitt C, et al.: Practice guidelines for central venous access: a report by the American Society of Anesthesiologists Task Force on Central Venous Access. Anesthesiology 2012, 116(3):539–573. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
