

Retention outcomes and drivers of loss among HIV-exposed and infected infants in Uganda: a retrospective cohort study
- PMID: 30134851
- PMCID: PMC6104004
- DOI: 10.1186/s12879-018-3275-6
Retention outcomes and drivers of loss among HIV-exposed and infected infants in Uganda: a retrospective cohort study
Abstract
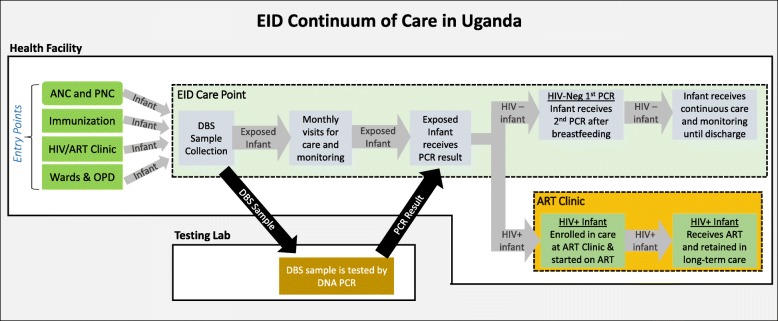
Background: Uganda's HIV Early Infant Diagnosis (EID) program rapidly scaled up testing of HIV-exposed infants (HEI) in its early years. However, little was known about retention outcomes of HEI after testing. Provision of transport refunds to HEI caregivers was piloted at 3 hospitals to improve retention. This study was conducted to quantify retention outcomes of tested HEI, identify factors driving loss-to-follow-up, and assess the effect of transport refunds on HEI retention.
Methods: This mixed-methods study included 7 health facilities- retrospective cohort review at 3 hospitals and qualitative assessment at all facilities. The cohort comprised all HEI tested from September-2007 to February-2009. Retention data was collected manually at each hospital. Qualitative methods included health worker interviews and structured clinic observation. Qualitative data was synthesized, analyzed and triangulated to identify factors driving HEI loss-to-follow-up.
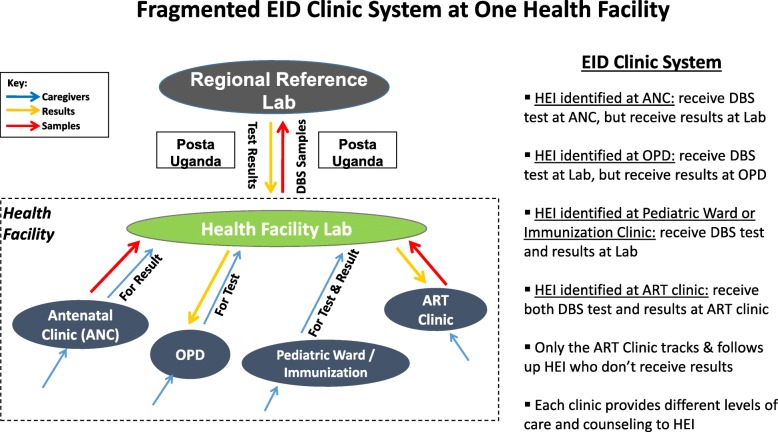
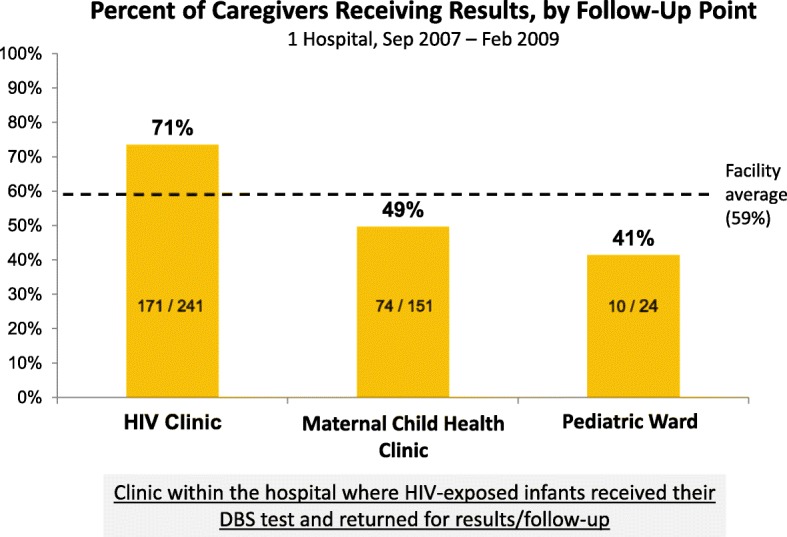
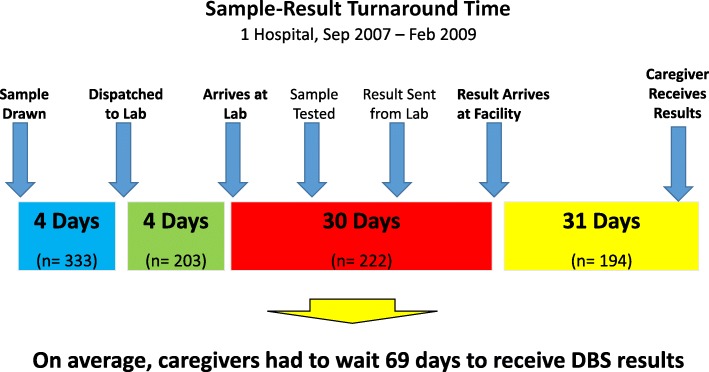
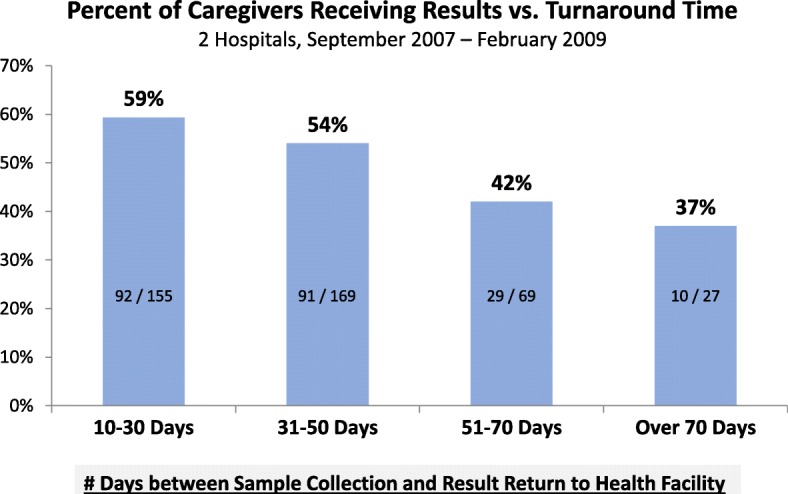
Results: The cohort included 1268 HEI, with 244 testing HIV-positive. Only 57% (718/1268) of tested HEI received results. The transport refund pilot increased the percent of HEI caregivers receiving test results from 54% (n = 763) to 58% (n = 505) (p = .08). HEI were tested at late ages (Mean = 7.0 months, n = 1268). Many HEI weren't tested at all: at 1 hospital, only 18% (67/367) of HIV+ pregnant women brought their HEI for testing after birth. Among HIV+ infants, only 40% (98/244) received results and enrolled at an ART Clinic. Of enrolled HIV+ infants, only 43% (57/98) were still active in chronic care. 36% (27/75) of eligible HIV+ infants started ART. Our analysis identified 6 categories of factors driving HEI loss-to-follow-up: fragmentation of EID services across several clinics, with most poorly equipped for HEI care/follow-up; poor referral mechanisms and data management systems; inconsistent clinical care; substandard counseling; poor health worker knowledge of EID; long sample-result turnaround times.
Discussion: The poor outcomes for HEI and HIV+ infants have highlighted an urgent need to improve retention and linkage to care. To address the identified gaps, Uganda's Ministry of Health and the Clinton Health Access Initiative developed a new implementation model, shifting EID from a lab-based diagnostic service to an integrated clinic-based chronic care model. This model was piloted at 21 facilities. An evaluation is needed.
Keywords: Early infant diagnosis; HIV; HIV-exposed infant; Linkage to care; Pediatric HIV; Prevention of mother-to-child transmission; Retention; Testing; Uganda.
Conflict of interest statement
Ethics approval and consent to participate
This study was reviewed and approved by the Mildmay Uganda Research and Ethics Committee (MUREC). Confidentiality of patients in the retrospective cohort was ensured through use of serial identifier numbers in data capture tools. Informed written consent was obtained from all interviewed health workers.
Consent for publication
Not applicable.
Competing interests
The authors of this study declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures




Similar articles
-
Uganda's "EID Systems Strengthening" model produces significant gains in testing, linkage, and retention of HIV-exposed and infected infants: An impact evaluation.PLoS One. 2021 Feb 4;16(2):e0246546. doi: 10.1371/journal.pone.0246546. eCollection 2021. PLoS One. 2021. PMID: 33539425 Free PMC article.
-
Use of peers, community lay persons and Village Health Team (VHT) members improves six-week postnatal clinic (PNC) follow-up and Early Infant HIV Diagnosis (EID) in urban and rural health units in Uganda: A one-year implementation study.BMC Health Serv Res. 2015 Dec 15;15:555. doi: 10.1186/s12913-015-1213-5. BMC Health Serv Res. 2015. PMID: 26666331 Free PMC article.
-
Rapid antiretroviral therapy initiation following rollout of point-of-care early infant diagnosis testing, Uganda, 2018-2021.AIDS Res Ther. 2024 May 15;21(1):31. doi: 10.1186/s12981-024-00613-8. AIDS Res Ther. 2024. PMID: 38750529 Free PMC article.
-
Improved access to early infant diagnosis is a critical part of a child-centric prevention of mother-to-child transmission agenda.AIDS. 2013 Nov;27 Suppl 2:S197-205. doi: 10.1097/QAD.0000000000000104. AIDS. 2013. PMID: 24361629 Review.
-
Interventions to increase early infant diagnosis of HIV infection: A systematic review and meta-analysis.PLoS One. 2022 Feb 25;17(2):e0258863. doi: 10.1371/journal.pone.0258863. eCollection 2022. PLoS One. 2022. PMID: 35213579 Free PMC article.
Cited by
-
Early infant diagnosis testing for HIV in a hard-to-reach fishing community in Uganda.PLoS One. 2023 Jun 7;18(6):e0268416. doi: 10.1371/journal.pone.0268416. eCollection 2023. PLoS One. 2023. PMID: 37285359 Free PMC article.
-
The outcome of prevention of mother-to-child transmission of HIV infection at King Abdulaziz University Hospital, Western Region of Saudi Arabia: A Descriptive Study.Saudi Med J. 2021 Sep;42(9):1009-1016. doi: 10.15537/smj.2021.42.9.20200789. Saudi Med J. 2021. PMID: 34470840 Free PMC article.
-
A scoping review on HIV early infant diagnosis among HIV exposed infants, ART use and adherence in Tanzania.BMC Infect Dis. 2023 Dec 11;23(1):868. doi: 10.1186/s12879-023-08868-8. BMC Infect Dis. 2023. PMID: 38082235 Free PMC article.
-
Uganda's "EID Systems Strengthening" model produces significant gains in testing, linkage, and retention of HIV-exposed and infected infants: An impact evaluation.PLoS One. 2021 Feb 4;16(2):e0246546. doi: 10.1371/journal.pone.0246546. eCollection 2021. PLoS One. 2021. PMID: 33539425 Free PMC article.
-
Measuring retention in care for HIV-positive pregnant women in Prevention of Mother-to-Child Transmission of HIV (PMTCT) option B+ programs: the Mozambique experience.BMC Public Health. 2020 Mar 12;20(1):322. doi: 10.1186/s12889-020-8406-5. BMC Public Health. 2020. PMID: 32164601 Free PMC article.
References
-
- UNAIDS. Global Report: UNAIDS Report on the Global AIDS Epidemic. 2010. Geneva, Switzerland. Accessed from http://www.unaids.org/globalreport/documents/20101123_GlobalReport_full_....
-
- UNAIDS. Fact Sheet: Global HIV Statistics. 2017. Geneva, Switzerland. Accessed from http://www.unaids.org/sites/default/files/media_asset/UNAIDS_FactSheet_e....
-
- UNAIDS. 90-90-90 An Ambitious Treatment Target to Help End the AIDS Epidemic. 2014. Geneva, Switzerland. Accessed from http://www.unaids.org/sites/default/files/media_asset/90-90-90_en_0.pdf.
-
- UNAIDS, Uganda AIDS Commission. Uganda HIV Prevention Response and Modes of Transmission Analysis. 2009. Kampala, Uganda. Accessed from http://web.worldbank.org/archive/website01390/WEB/IMAGES/UGANDAMO.PDF.
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
