

Pharmacodynamics of atabecestat (JNJ-54861911), an oral BACE1 inhibitor in patients with early Alzheimer's disease: randomized, double-blind, placebo-controlled study
- PMID: 30134967
- PMCID: PMC6106931
- DOI: 10.1186/s13195-018-0415-6
Pharmacodynamics of atabecestat (JNJ-54861911), an oral BACE1 inhibitor in patients with early Alzheimer's disease: randomized, double-blind, placebo-controlled study
Abstract
Background: β-Secretase enzyme (BACE) inhibition has been proposed as a priority treatment mechanism for Alzheimer's disease (AD), but treatment initiation may need to be very early. We present proof of mechanism of atabecestat (also known as JNJ-54861911), an oral BACE inhibitor for the treatment of AD, in Caucasian and Japanese populations with early AD who do not show signs of dementia.
Methods: In two similarly designed phase I studies, a sample of amyloid-positive elderly patients comprising 45 Caucasian patients with early AD diagnosed as preclinical AD (n = 15, Clinical Dementia Rating [CDR] = 0) or with mild cognitive impairment due to AD (n = 30, CDR = 0.5) and 18 Japanese patients diagnosed as preclinical AD (CDR-J = 0) were randomized 1:1:1 to atabecestat 10 or 50 mg or placebo (n = 6-8/treatment) daily for 4 weeks. Safety, pharmacokinetics (PK), and pharmacodynamics (PD) (i.e., reduction of cerebrospinal fluid [CSF] amyloid beta 1-40 [Aβ1-40] levels [primary endpoint] and effect on other AD biomarkers) of atabecestat were evaluated.
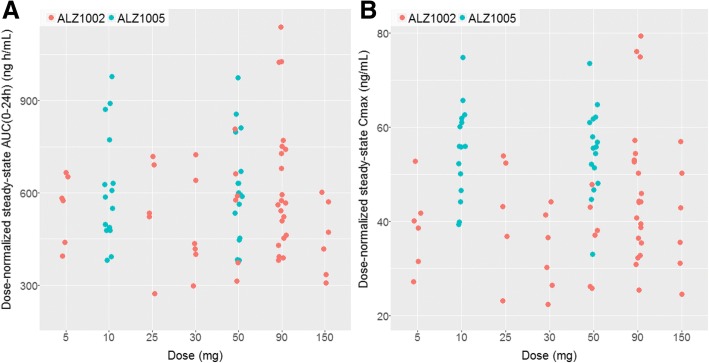
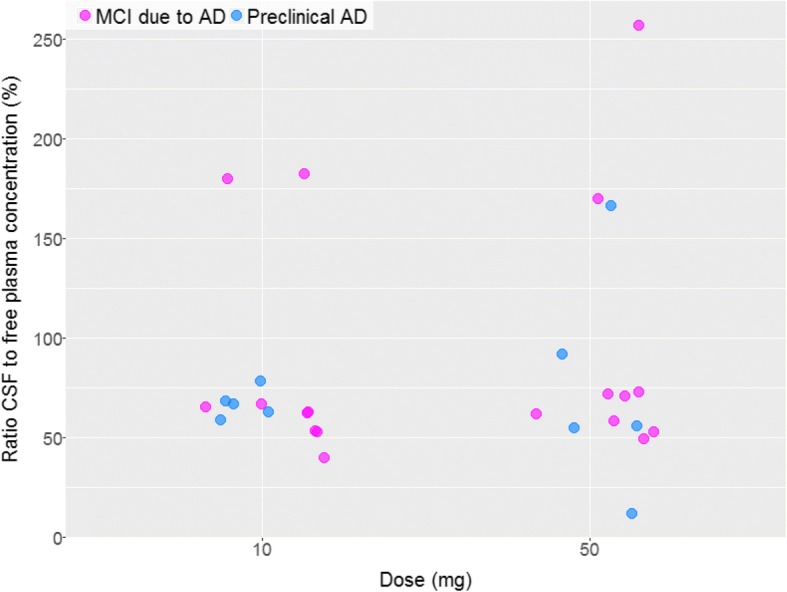
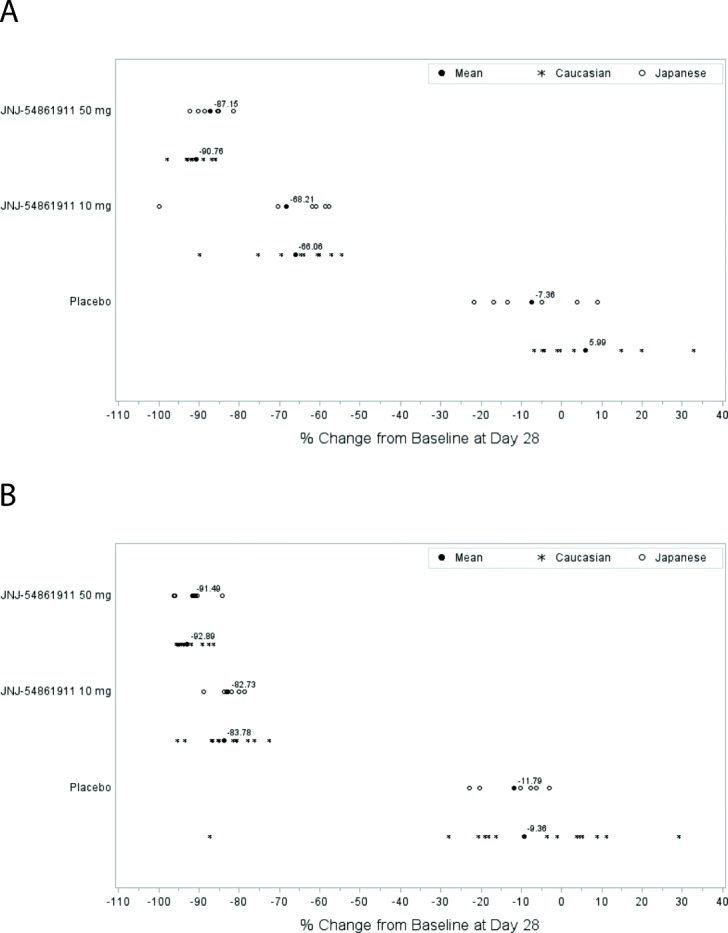
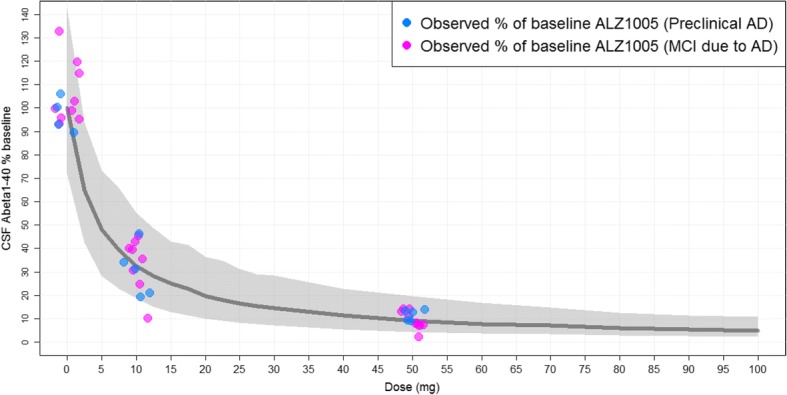
Results: In both populations, atabecestat was well tolerated and characterized by linear PK and high central nervous system penetrance of unbound drug. Atabecestat significantly reduced CSF Aβ1-40 levels from baseline at day 28 in both the 10-mg (67-68%) and 50-mg (87-90%) dose groups compared with placebo. For Caucasians with early AD, the least squares mean differences (95% CI) were - 69.37 (- 72.25; - 61.50) and - 92.74 (- 100.08; - 85.39), and for Japanese with preclinical AD, they were - 62.48 (- 78.32; - 46.64) and - 80.81 (- 96.13; - 65.49), respectively. PK/PD model simulations confirmed that once-daily 10 mg and 50 mg atabecestat can attain 60-70% and 90% Aβ1-40 reductions, respectively. The trend of the reduction was similar across the Aβ1-37, Aβ1-38, and Aβ1-42 fragments in both atabecestat dose groups, consistent with Aβ1-40. CSF amyloid precursor protein fragment (sAPPβ) levels declined from baseline, regardless of patient population, whereas CSF sAPPα levels increased compared with placebo. There were no relevant changes in either CSF total tau or phosphorylated tau 181P over a 4-week treatment period.
Conclusions: JNJ-54861911 at 10 and 50 mg daily doses after 4 weeks resulted in mean CSF Aβ1-40 reductions of 67% and up to 90% in both Caucasian and Japanese patients with early stage AD, confirming results in healthy elderly adults.
Trial registration: ALZ1005: ClinicalTrials.gov, NCT01978548. Registered on 7 November 2013. ALZ1008: ClinicalTrials.gov, NCT02360657. Registered on 10 February 2015.
Keywords: Alzheimer’s disease; Amyloid; Atabecestat; Aβ processing; BACE1 inhibitor; JNJ-54861911; PK/PD relationship.
Conflict of interest statement
Ethics approval and consent to participate
The study protocol and amendments were approved by the appropriate independent ethics committees/institutional review boards. Written informed consent was obtained from all participants before their participation. All study procedures followed were in accordance with current International Conference on Harmonization guidelines on good clinical practice, applicable regulatory and country-specific requirements, and the principles of the Declaration of Helsinki.
Consent for publication
Not applicable.
Competing interests
All authors, except ABH, NA, SE, JMG, MBa, and MBo, report receiving personal fees (employment) from Janssen Research & Development, a Division of Janssen Pharmaceutica N.V., Beerse, Belgium, or Janssen Research & Development, LLC, Raritan, NJ, USA, or Janssen Research and Development LLC, Titusville, NJ, USA, or Janssen Pharmaceutical K.K., Tokyo, Japan, and all own stock/stock options in the company. JRS is a former employee of Janssen Pharmaceutica NV and is currently affiliated with the University of Antwerp with a research advisory role at the Reference Center for Biological Markers of Dementia (BIODEM), Institute Born-Bunge, University of Antwerp, Antwerp, Belgium, and collects no consulting fees and receives no research funding. ABH is employed at Sahlgrenska University Hospital, Mölndal, Sweden, and has no disclosures to declare. NA is employed at Karolinska Institutet, Department of Neurobiology, Care Sciences and Society, Center for Alzheimer Research, Division of Neurogeriatrics, Stockholm, Sweden, and has no disclosures to declare. SE is employed at the Department of Biomedical Sciences, University of Antwerp, Antwerp, Belgium, and at the Department of Neurology and Memory Clinic, Hospital Network Antwerp (ZNA) Middelheim and Hoge Beuken, Antwerp, Belgium, and reports receiving research funding from Janssen Pharmaceutica N.V. and ADx Neurosciences (paid to institution). JMG is an employee of San Carlos Hospital Clinic, Universidad Complutense, Madrid, Spain, and receives salary as chief editor of a scientific journal indexed in Medline and Journal Citation Reports. MBa is an employee of Hospital Universitari i Politecnic La Fe, Valencia, Spain, and has no disclosures to declare. MBo is an employee of Fundació ACE, Institut Català de Neurociències Aplicades, Barcelona, Spain, and consults for Araclon, AstraZeneca, Grifols, Janssen, Kyowa Kirin, Lilly, MSD, Nutricia, Roche, Schwabe, and Servier. MBo has received fees for lectures from Araclon Biotech, Biogen, Grifols, Krka, Nutricia, Roche, and Schwabe, and reports receiving research funding from Araclon Biotech, Bioiberica, Grifols, Krka, Lilly, Merck, Piramal, Nutricia, Roche, Fundació Bancaria la Caixa, Carlos III Health Institute, the European Commission Horizon 2020 program, European Federation of Pharmaceutical Industries and Associations Innovative Medicines Initiative, and the European Research Area ERA-NET program.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Sperling RA, Aisen PS, Beckett LA, Bennett DA, Craft S, Fagan AM, et al. Toward defining the preclinical stages of Alzheimer’s disease: recommendations from the National Institute on Aging-Alzheimer’s Association workgroups on diagnostic guidelines for Alzheimer’s disease. Alzheimers Dement. 2011;7:280–292. doi: 10.1016/j.jalz.2011.03.003. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
