

Characteristics of undiagnosed diseases network applicants: implications for referring providers
- PMID: 30134969
- PMCID: PMC6106923
- DOI: 10.1186/s12913-018-3458-2
Characteristics of undiagnosed diseases network applicants: implications for referring providers
Abstract
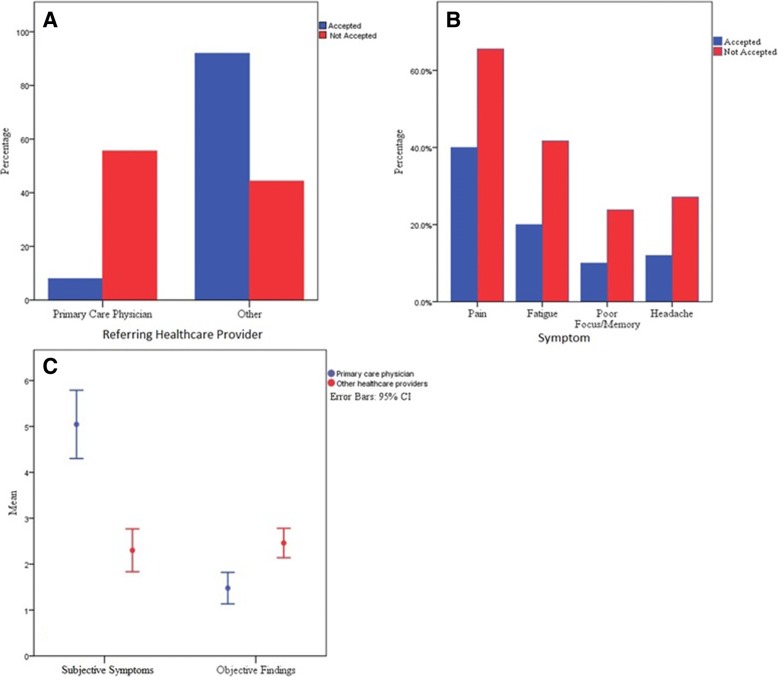
Background: The majority of undiagnosed diseases manifest with objective findings that warrant further investigation. The Undiagnosed Diseases Network (UDN) receives applications from patients whose symptoms and signs have been intractable to diagnosis; however, many UDN applicants are affected primarily by subjective symptoms such as pain and fatigue. We sought to characterize presenting symptoms, referral sources, and demographic factors of applicants to the UDN to identify factors that may determine application outcome and potentially differentiate between those with undiagnosed diseases (with more objective findings) and those who are less likely to have an undiagnosed disease (more subjective symptoms).
Methods: We used a systematic retrospective review of 151 consecutive Not Accepted and 50 randomly selected Accepted UDN applications. The primary outcome was whether an applicant was Accepted, or Not Accepted, and, if accepted, whether or not a diagnosis was made. Objective and subjective symptoms and information on prior specialty consultations were collected from provider referral letters. Demographic data and decision data on network acceptance were gathered from the UDN online portal.
Results: Fewer objective findings and more subjective symptoms were found in the Not Accepted applications. Not Accepted referrals also were from older individuals, reported a shorter period of illness, and were referred to the UDN by their primary care physicians. All of these differences reached statistical significance in comparison with Accepted applications. The frequency of subspecialty consults for diagnostic purposes prior to UDN application was similar in both groups.
Conclusions: The preponderance of subjective and lack of objective findings in the Not Accepted applications distinguish these from applicants that are accepted for evaluation and diagnostic efforts through the UDN. Not Accepted applicants are referred primarily by their primary care providers after multiple specialist consultations fail to yield answers. Distinguishing between patients with undiagnosed diseases with objective findings and those with primarily subjective findings can delineate patients who would benefit from further diagnostic processes from those who may have functional disorders and need alternative pathways for management of their symptoms.
Trial registration: clinicaltrials.gov NCT02450851 , posted May 21st 2015.
Keywords: Genomics; Health policy; Medically unexplained physical symptoms; Medically unexplained symptoms; Undiagnosed diseases.
Conflict of interest statement
Ethics approval and consent to participate
All applicants provided electronic informed consent with electronic signature as approved by the National Human Genome Research Institute Institutional Review Board under research protocol 15-HG-0130.
Consent for publication
Consent for research and publication is included in the electronic informed consent as approved by the National Human Genome Research Institute Institutional Review Board under research protocol 15-HG-0130.
Competing interests
The named authors of this work report no conflicts of interest. Members of the Undiagnosed Diseases Network report the following conflicts of interest: E.A.A. is an advisor to and stockholder in Personalis Inc. D.P.B. is a founder and chief medical officer of Envision Genomics, medical director of Smith Family Clinic LLC, assistant director of Clinical Services Laboratory LLC, and a scientific advisory board member of Genomics England. C.M.E. is a fulltime faculty member of Baylor College of Medicine and provides services as chief medical officer and chief quality officer to Baylor Genetics Laboratory through a professional services agreement. P.G.F. is an associate editor of the Journal of Pediatrics (Elsevier) and a paid consultant. D.B.G. owns equity in two precision medicine companies, Pairnomix and Clarus/EpiPM. J.E.P. is an employee of the Department of Molecular and Human Genetics at Baylor College of Medicine, which has entered a joint venture with Baylor Genetics Laboratory. J.A.R. is a member of the Department of Molecular and Human Genetics at Baylor College of Medicine, which derives revenue from clinical genetic testing offered by Baylor Genetics. M.S.C. is a laboratory director for the HudsonAlpha Clinical Services Lab LLC, which performs fee-for-service clinical laboratory testing. D.A.S. is a member of the Clinical Advisory Board of Baylor Genetics and works for the Department of Molecular and Human Genetics at Baylor College of Medicine, which derives revenue from genetic analyses offered through Baylor Genetics. E.K.S. received honoraria and consulting fees from Merck, grant support and consulting fees from GlaxoSmithKline, and honoraria and travel support from Novartis. P.A.W. is a contract employee for Baylor Genetics, a clinical laboratory that derives income from whole-exome sequencing and other genetic testing.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- https://globalgenes.org. Rare Disease Statistics 2015.
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
