

Atherogenic index of plasma (AIP): a novel predictive indicator for the coronary artery disease in postmenopausal women
- PMID: 30134981
- PMCID: PMC6106932
- DOI: 10.1186/s12944-018-0828-z
Atherogenic index of plasma (AIP): a novel predictive indicator for the coronary artery disease in postmenopausal women
Abstract
Background: Dyslipidemia is one of the most important factors for coronary artery disease (CAD). Atherogenic index of plasma (AIP) is a novel indicator involved in dyslipidemia. However, the relation between AIP and CAD in postmenopausal women remains unclear. We hypotheses that AIP is a strong predictive indicator of CAD in postmenopausal women.
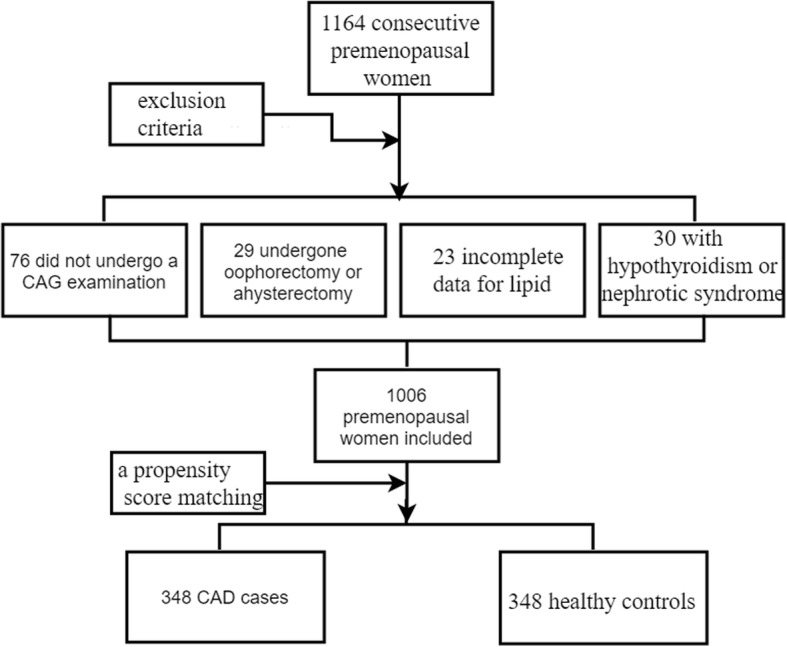
Methods: A propensity score matching case-control study including 348 postmenopausal CAD cases and 348 controls was conducted in the present study.
Results: Compared with controls, CAD patients had higher levels of total cholesterol (TC), triglyceride (TG), low-density lipoprotein cholesterol (LDL-C) and apolipoprotein B (APOB), but lower high-density lipoprotein cholesterol (HDL-C) and apolipoprotein A-1 (APOA-1). The values of nontraditional lipid profiles, including non-HDL-C, TC/HDL-C, LDL-C/HDL-C, non-HDL-C/HDL-C (atherogenic index, AI), TC∗TG∗LDL/HDL-C (lipoprotein combine index, LCI), log(TG/HDL-C) (atherogenic index of plasma, AIP) and APOB/APOA-1 were all significantly higher in the CAD patients. The results of Pearson correlation analyses showed AIP was positively and significantly correlated with TC (r = 0.092, P < 0.001), TG (r = 0.775, P = 0.015), APOB (r = 0.140, P < 0.001), non-HDL-C (r = 0.295, P < 0.001), TC/HDL-C (r = 0.626, P < 0.001), LDL-C/HDL-C (r = 0.469, P < 0.001), AI (r = 0.626, P < 0.001), LCI (r = 0.665, P < 0.001), APOB/APOA-1(r = 0.290, P < 0.001) and was negatively correlated with APOA-1 (r = - 0.278, P < 0.001) and HDL-C (r = - 0.665, P < 0.001). In the multivariate logistic regression analysis, AIP was an independent predictor of CAD. After adjusting for the traditional clinical prognostic factors including diabetes and hypertension, we found AIP could be an independent risk factor for CAD (odds ratio [OR], 3.290; 95% confidence interval [CI], 1.842-5.877, P < 0.001). After adjusting for multiple clinical factors include diabetes, hypertension, smoking, heart ratio, fasting blood glucose, we found AIP also could a powerful risk factor, OR = 3.619, 95%CI (2.003-6.538), P < 0.001.
Conclusion: The present study indicated that AIP might be a strong marker for predicting the risk of CAD in postmenopausal women.
Keywords: Atherogenic index of plasma; Coronary artery disease; Lipids; Postmenopausal women.
Conflict of interest statement
Ethics approval and consent to participate
The research protocol was approved by the ethics committee or review committee of the First Affiliated Hospital of Xinjiang Medical University. Because the study was a retrospective cohort study based on real-world situations, there was no need to obtain informed consent from the patients.
Consent for publication
All authors aggree to publish this work.
Competing interests
No potential conflicts of interest relevant to this article were reported by any of the authors. None of the funding sources played a role in the design, collection, analysis or interpretation of the data or in the decision to submit the manuscript for publication. The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
-
- Aatola H, Hutri-Kähönen N, Juonala M, Laitinen TT, Pahkala K, Mikkilä V, Telama R, Koivistoinen T, Lehtimäki T, Viikari JS, Raitakari OT, Kähönen M. Prospective relationship of change in ideal cardiovascular health status and arterial stiffness: the cardiovascular risk in young Finns study. J Am Heart Assoc. 2014;3(2):e000532. doi: 10.1161/JAHA.113.000532. - DOI - PMC - PubMed
-
- Folsom AR, Yatsuya H, Nettleton JA, Lutsey PL, Cushman M. Rosamond WD; ARIC study Investigators.Community prevalence of ideal cardiovascular health, by the American Heart Association definition, and relationship with cardiovascular disease incidence. J Am Coll Cardiol. 2011;57(16):1690–1696. doi: 10.1016/j.jacc.2010.11.041. - DOI - PMC - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
