

Blood Culture Turnaround Time in U.S. Acute Care Hospitals and Implications for Laboratory Process Optimization
- PMID: 30135230
- PMCID: PMC6258864
- DOI: 10.1128/JCM.00500-18
Blood Culture Turnaround Time in U.S. Acute Care Hospitals and Implications for Laboratory Process Optimization
Abstract
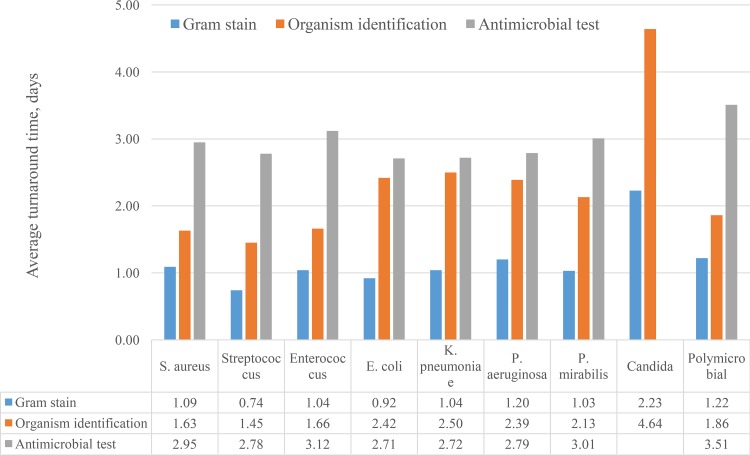
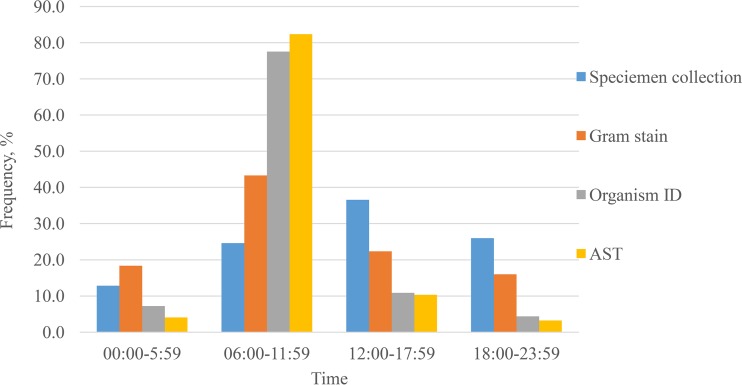
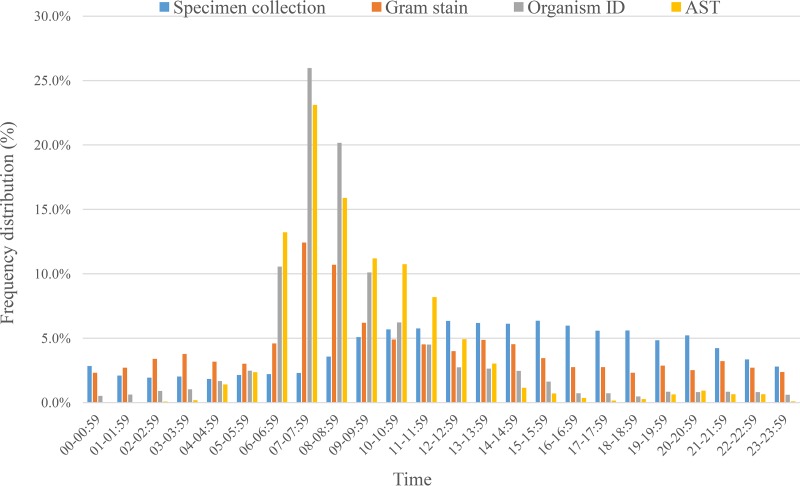
The rapid identification of blood culture isolates and antimicrobial susceptibility test (AST) results play critical roles for the optimal treatment of patients with bloodstream infections. Whereas others have looked at the time to detection in automated culture systems, we examined the overall time from specimen collection to actionable test results. We examined four points of time, namely, blood specimen collection, Gram stain, organism identification (ID), and AST reports, from electronic data from 13 U.S. hospitals for the 11 most common, clinically significant organisms in septic patients. We compared the differences in turnaround times and the times from when specimens were collected and the results were reported in the 24-h spectrum. From January 2015 to June 2016, 165,593 blood specimens were collected, of which, 9.5% gave positive cultures. No matrix-assisted laser desorption ionization-time of flight (MALDI-TOF) mass spectrometry was used during the study period. Across the 10 common bacterial isolates (n = 6,412), the overall median (interquartile range) turnaround times were 0.80 (0.64 to 1.08), 1.81 (1.34 to 2.46), and 2.71 (2.46 to 2.99) days for Gram stain, organism ID, and AST, respectively. For all positive cultures, approximately 25% of the specimens were collected between 6:00 a.m. and 11:59 a.m. In contrast, more of the laboratory reporting times were concentrated between 6:00 a.m. and 11:59 a.m. for Gram stain (43%), organism ID (78%), and AST (82%), respectively (P < 0.001). The overall average turnaround times from specimen collection for Gram stain, organism ID, and AST were approximately 1, 2, and 3 days, respectively. The laboratory results were reported predominantly in the morning hours. Laboratory automation and work flow optimization may play important roles in reducing the microbiology result turnaround time.
Keywords: blood culture; clinical microbiology; laboratory automation; laboratory workflow.
Copyright © 2018 American Society for Microbiology.
Figures
References
-
- Rhodes A, Evans LE, Alhazzani W, Levy MM, Antonelli M, Ferrer R, Kumar A, Sevransky JE, Sprung CL, Nunnally ME, Rochwerg B, Rubenfeld GD, Angus DC, Annane D, Beale RJ, Bellinghan GJ, Bernard GR, Chiche J-D, Coopersmith C, De Backer DP, French CJ, Fujishima S, Gerlach H, Hidalgo JL, Hollenberg SM, Jones AE, Karnad DR, Kleinpell RM, Koh Y, Lisboa TC, Machado FR, Marini JJ, Marshall JC, Mazuski JE, McIntyre LA, McLean AS, Mehta S, Moreno RP, Myburgh J, Navalesi P, Nishida O, Osborn TM, Perner A, Plunkett CM, Ranieri M, Schorr CA, Seckel MA, Seymour CW, Shieh L, Shukri KA, et al. 2017. Surviving sepsis campaign: international guidelines for management of sepsis and septic shock: 2016. Intensive Care Med 43:304–377. doi:10.1007/s00134-017-4683-6. - DOI - PubMed
-
- Diamantis S, Rioux C, Bonnal C, Farfour É, Papy E, Andremont A, Yeni P, Bouvet É, Lucet J-C. 2012. Suitability of initial antibiotic therapy for the treatment of bloodstream infections and the potential role of antibiotic management teams in improving it. Eur J Clin Microbiol Infect Dis 31:1667–1671. doi:10.1007/s10096-011-1491-8. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
