

Barriers and facilitators for the implementation of blended psychotherapy for depression: A qualitative pilot study of therapists' perspective
- PMID: 30135779
- PMCID: PMC6096333
- DOI: 10.1016/j.invent.2018.01.002
Barriers and facilitators for the implementation of blended psychotherapy for depression: A qualitative pilot study of therapists' perspective
Abstract
Introduction: Blended therapies (BT) combine face-to-face (f2f) sessions with internet- and mobile-based interventions (IMIs). However, the use of blended interventions in routine care is still rare and depends on the acceptance of key health care professionals such as the therapists. Little is yet known about the therapists' perspective on and experiences with blended approaches. The aim of this pilot study was to identify barriers and facilitators, as perceived by psychotherapists, for implementing a blended therapy for depression.
Methods: Semi-structured expert interviews were conducted with five therapists, who were part of the German study arm of the FP7-project E-Compared (www.e-compared.eu). All patients (N = 173) were treated in the context of a registered RCT (DRKS00006866) in which the clinical and cost-effectiveness of BT for depression, consisting of ten internet- and mobile-based cognitive behavioral therapy modules and six f2f sessions, was compared to the treatment usually provided by general practitioners. To identify barriers and facilitators an interview guide based on the theoretical domains framework (TDF) was developed. The interviews were audio-recorded, transcribed verbatim and analyzed using a qualitative content analysis by two independent coders.
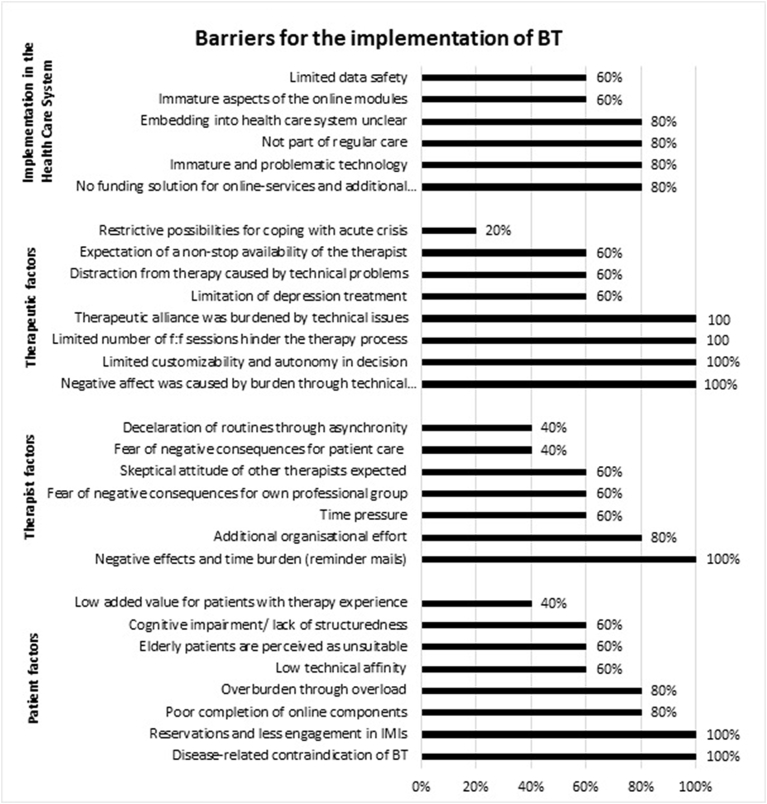
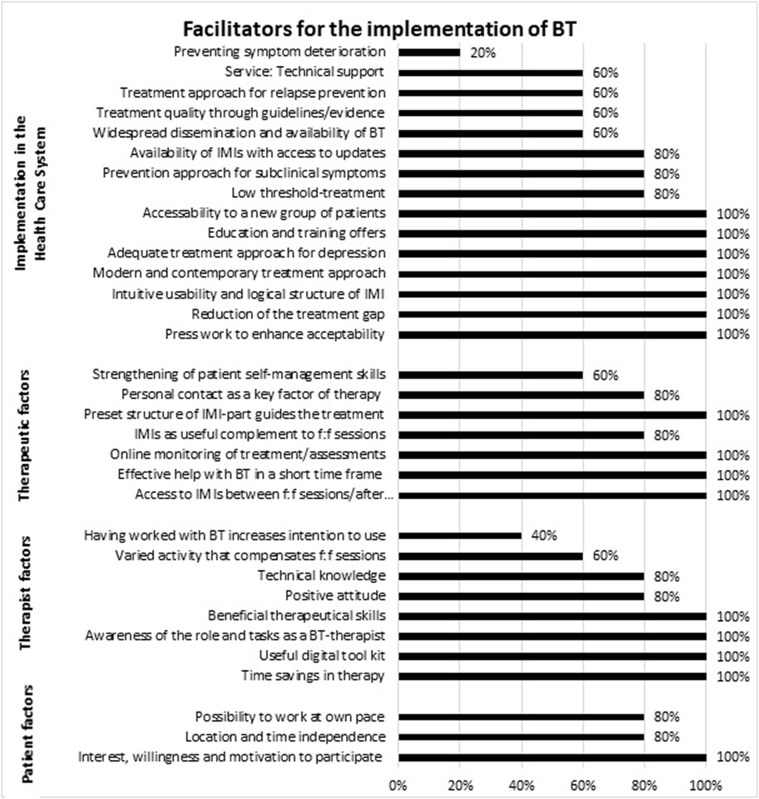
Results: The results revealed 29 barriers and 33 facilitators, which are hindering or enabling factors on the levels of 'implementation in the health care system', 'therapy', 'therapists' and 'patients'. Key barriers stated by all therapists were 'Limited customizability and autonomy of decisions concerning blending the therapy' (number of statements, k = 44); 'Disease-related contraindications for BT' (k = 25); 'Negative affect was caused by burden through technical problems' (k = 18); 'Limited number of f2f sessions hindered the therapy process'; and 'Establishment of therapeutic alliance was burdened by technical issues' (each k = 15). Key facilitators stated by all therapists were: 'Patients' interest, willingness and motivation to participate' (k = 22); 'Patients' access to online content between f2f sessions and after therapy end' (k = 20); 'Preset structure of IMI-part guided the treatment course of BT' (k = 18); and 'Effective help with BT in a short time frame' (k = 15), as well as 'Reduction of the treatment gap' (k = 13).
Discussion: Therapists supported the implementation of BT for depression. Results indicated the consideration of a wide range of determinants: among others, the possibility of individualizing the treatment; the autonomy of decision making in respect to the ratio and number of online and f2f sessions; the necessity of providing training; the need to develop a concept of embedding BT in the health care system and funding the additional effort; and the use of sophisticated technical solutions.
Keywords: Barriers; Blended therapy; Depression; Facilitators; Qualitative study; Therapists' view.
Figures
References
-
- Alexander C., Fraser J. General practitioners' management of patients with mental health conditions: the views of general practitioners working in rural north-western New South Wales. Aust. J. Rural Health. 2008;16(6):363–369. - PubMed
-
- Alkhaldi B., Sahama T., Huxley C., Gajanayake R. Studies in Health Technology and Informatics. Vol 205. 2014. Barriers to implementing eHealth: a multi-dimensional perspective; pp. 875–879. - PubMed
-
- Alonso J., Angermeyer M.C., Bernert S. Prevalence of mental disorders in Europe: results from the European study of the epidemiology of mental disorders (ESEMeD) project. Acta Psychiatr. Scand. Suppl. 2004;420:21–27. - PubMed
-
- Andersson G., Hedman E. Effectiveness of guided internet-based cognitive behavior therapy in regular clinical settings. Verhaltenstherapie. 2013;23(3):140–148.
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
