

Impact of medication reconciliation for improving transitions of care
- PMID: 30136718
- PMCID: PMC6513651
- DOI: 10.1002/14651858.CD010791.pub2
Impact of medication reconciliation for improving transitions of care
Abstract
Background: Transitional care provides for the continuity of care as patients move between different stages and settings of care. Medication discrepancies arising at care transitions have been reported as prevalent and are linked with adverse drug events (ADEs) (e.g. rehospitalisation).Medication reconciliation is a process to prevent medication errors at transitions. Reconciliation involves building a complete list of a person's medications, checking them for accuracy, reconciling and documenting any changes. Despite reconciliation being recognised as a key aspect of patient safety, there remains a lack of consensus and evidence about the most effective methods of implementing reconciliation and calls have been made to strengthen the evidence base prior to widespread adoption.
Objectives: To assess the effect of medication reconciliation on medication discrepancies, patient-related outcomes and healthcare utilisation in people receiving this intervention during care transitions compared to people not receiving medication reconciliation.
Search methods: We searched CENTRAL, MEDLINE, Embase, seven other databases and two trials registers on 18 January 2018 together with reference checking, citation searching, grey literature searches and contact with study authors to identify additional studies.
Selection criteria: We included only randomised trials. Eligible studies described interventions fulfilling the Institute for Healthcare Improvement definition of medication reconciliation aimed at all patients experiencing a transition of care as compared to standard care in that institution. Included studies had to report on medication discrepancies as an outcome.
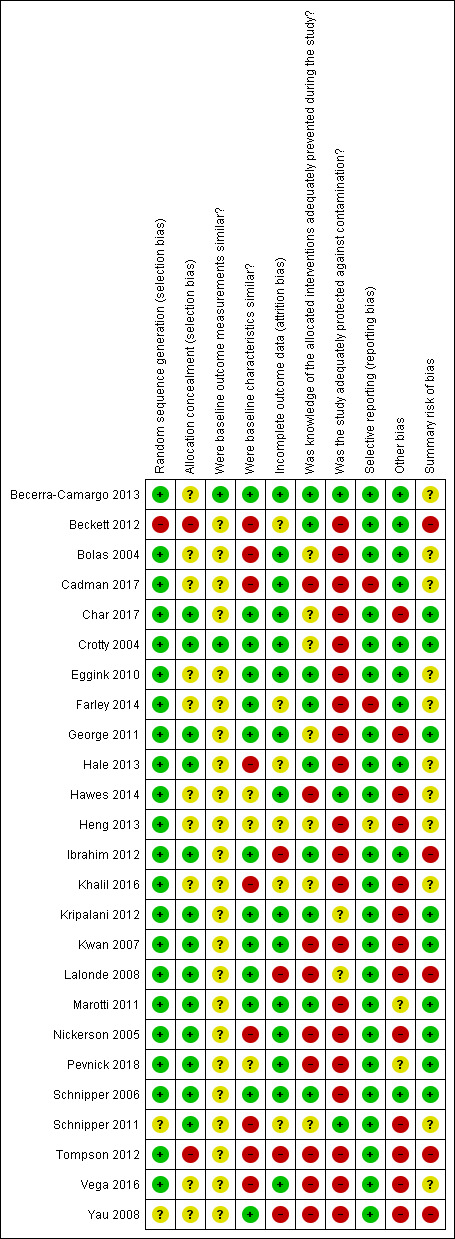
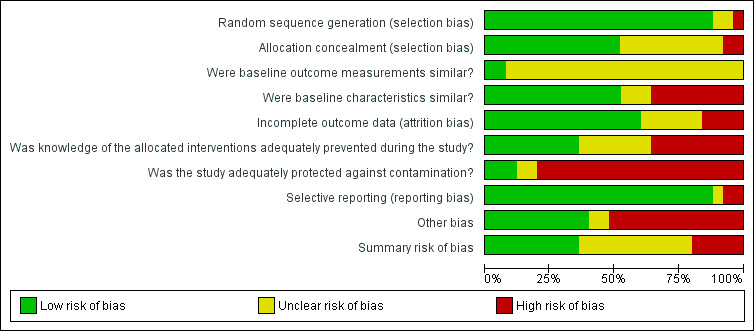
Data collection and analysis: Two review authors independently screened titles and abstracts, assessed studies for eligibility, assessed risk of bias and extracted data. Study-specific estimates were pooled, using a random-effects model to yield summary estimates of effect and 95% confidence intervals (CI). We used the GRADE approach to assess the overall certainty of evidence for each pooled outcome.
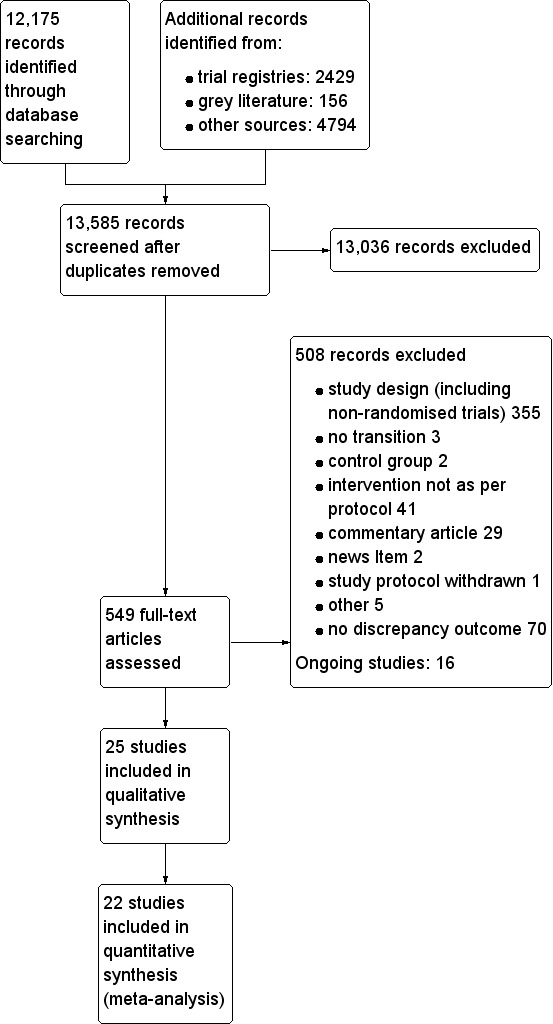
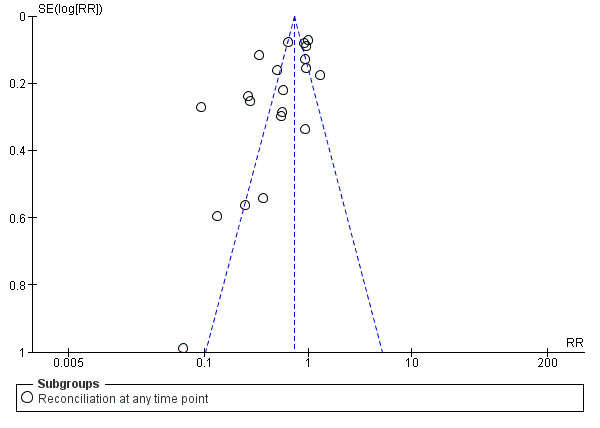
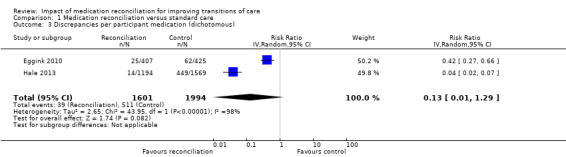
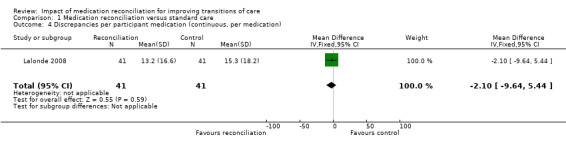
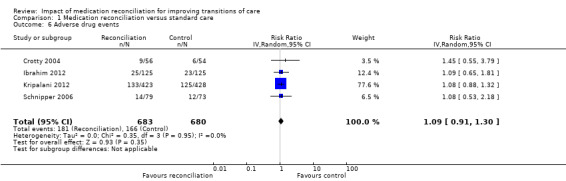
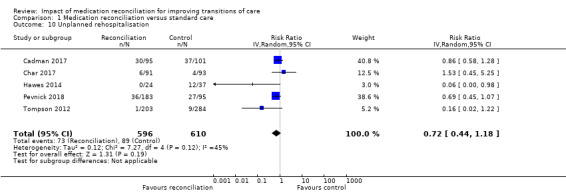
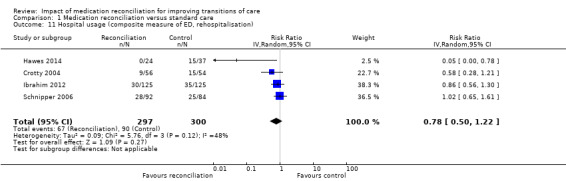
Main results: We identified 25 randomised trials involving 6995 participants. All studies were conducted in hospital or immediately related settings in eight countries. Twenty-three studies were provider orientated (pharmacist mediated) and two were structural (an electronic reconciliation tool and medical record changes). A pooled result of 20 studies comparing medication reconciliation interventions to standard care of participants with at least one medication discrepancy showed a risk ratio (RR) of 0.53 (95% CI 0.42 to 0.67; 4629 participants). The certainty of the evidence on this outcome was very low and therefore the effect of medication reconciliation to reduce discrepancies was uncertain. Similarly, reconciliation's effect on the number of reported discrepancies per participant was also uncertain (mean difference (MD) -1.18, 95% CI -2.58 to 0.23; 4 studies; 1963 participants), as well as its effect on the number of medication discrepancies per participant medication (RR 0.13, 95% CI 0.01 to 1.29; 2 studies; 3595 participants) as the certainty of the evidence for both outcomes was very low.Reconciliation may also have had little or no effect on preventable adverse drug events (PADEs) due to the very low certainty of the available evidence (RR 0.37. 95% CI 0.09 to 1.57; 3 studies; 1253 participants), with again uncertainty on its effect on ADE (RR 1.09, 95% CI 0.91 to 1.30; 4 studies; 1363 participants; low-certainty evidence). Evidence of the effect of the interventions on healthcare utilisation was conflicting; it probably made little or no difference on unplanned rehospitalisation when reported alone (RR 0.72, 95% CI 0.44 to 1.18; 5 studies; 1206 participants; moderate-certainty evidence), and had an uncertain effect on a composite measure of hospital utilisation (emergency department, rehospitalisation RR 0.78, 95% CI 0.50 to 1.22; 4 studies; 597 participants; very low-certainty evidence).
Authors' conclusions: The impact of medication reconciliation interventions, in particular pharmacist-mediated interventions, on medication discrepancies is uncertain due to the certainty of the evidence being very low. There was also no certainty of the effect of the interventions on the secondary clinical outcomes of ADEs, PADEs and healthcare utilisation.
Conflict of interest statement
PR: awarded a Cochrane Fellowship in 2012 by the Health Research Board (HRB) for the purpose of completing this review.
TG: none known.
RMcD: none known.
FB: none known.
CH: Received an honorarium as speaker to present results of an unrelated Cochrane review.
TF: none known.
Figures







Update of
References
References to studies included in this review
Becerra‐Camargo 2013 {published data only}
-
- Becerra‐Camargo J, Martinez‐Martinez F, Garcia‐Jimenez E. A multi centre, double‐blind, randomised, controlled, parallel‐group study of the effectiveness of a pharmacist‐acquired medication history in an emergency department. BMC Health Services Research 2013;13:337. [DOI: 10.1186/1472-6963-13-337; PUBMED: 23984830] - DOI - PMC - PubMed
Beckett 2012 {published data only}
-
- Beckett RD, Crank CW, Wehmeyer A. Effectiveness and feasibility of pharmacist‐led admission medication reconciliation for geriatric patients. Journal of Pharmacy Practice 2012;25(2):136‐41. - PubMed
Bolas 2004 {published data only}
-
- Bolas H, Brookes K, Scott M, McElnay J. Evaluation of a hospital‐based community liaison pharmacy service in Northern Ireland. Pharmacy World & Science : PWS 2004;26(2):114‐20. - PubMed
Cadman 2017 {published data only}
Char 2017 {published data only}
-
- Char CW, Yip AY, Kee KW, Lee ES, Chua AH. Effectiveness of pre‐consultation medication reconciliation service in reducing medication discrepancies during transition of care from hospital discharge to primary care setting in Singapore – a randomised controlled trial. Journal of Applied Pharmacy 2017;09(04):1‐8.
Crotty 2004 {published data only}
-
- Crotty M, Rowett D, Spurling L, Giles LC, Phillips PA. Does the addition of a pharmacist transition coordinator improve evidence‐based medication management and health outcomes in older adults moving from the hospital to a long‐term care facility? Results of a randomised, controlled trial. American Journal of Geriatric Pharmacotherapy 2004;2(4):257‐64. - PubMed
Eggink 2010 {published data only}
Farley 2014 {published and unpublished data}
George 2011 {published data only (unpublished sought but not used)}
-
- George LJW, Senturk‐Raif R, Hodgkinson MR, Emmerton M, Larmour I. Impact of a surgical preadmission clinic pharmacist on the quality of medication management from preadmission to discharge: a randomised controlled study. Journal of Pharmacy Practice and Research 2011;41(3):212‐6.
Hale 2013 {published and unpublished data}
Hawes 2014 {published data only}
-
- Hawes EM, Maxwell WD, White SF, Mangun J, Lin F‐C. Impact of an outpatient pharmacist intervention on medication discrepancies and health care resource utilization in post hospitalisation care transitions. Journal of Primary Care & Community Health 2014;5(1):14‐8. - PubMed
Heng 2013 {published data only}
-
- Heng ST, Lee JC. Medication reconciliation in outpatient hospital clinics. Annals of the Academy of Medicine Singapore 2013;42(9 Suppl):S7.
Ibrahim 2012 {published data only}
-
- Ibrahim OHM. Impact of clinical pharmacist intervention on decreasing incidence of preventable adverse drug events after hospital discharge. Advances in Pharmacoepidemiology & Drug Safety 2012;1(2):174.
Khalil 2016 {published and unpublished data}
-
- Khalil V, DeClifford JM, Lam S, Subramaniam A. Implementation and evaluation of a collaborative clinical pharmacist's medications reconciliation and charting service for admitted medical inpatients in a metropolitan hospital. Journal of Clinical Pharmacy and Therapeutics 2016;41(6):662‐6. - PubMed
Kripalani 2012 {published and unpublished data}
Kwan 2007 {published data only}
-
- Kwan Y, Fernandes OA, Nagge JJ, Wong GG, Huh J‐H, Hurn DA, et al. Pharmacist medication assessments in a surgical preadmission clinic. Archives of Internal Medicine 2007;167(10):1034‐40. - PubMed
Lalonde 2008 {published and unpublished data}
-
- Lalonde L, Lampron A, Vanier M, Levasseur P, Khaddag R, Chaar N. Effectiveness of a medication discharge plan for transitions of care from hospital to outpatient settings. American Journal of Health‐System Pharmacy 2008;65(15):1451‐7. - PubMed
Marotti 2011 {published and unpublished data}
-
- Marotti SB, Kerridge RK, Grimer MD. A randomised controlled trial of pharmacist medication histories and supplementary prescribing on medication errors in postoperative medications. Anaesthesia and Intensive Care 2011;39(6):1064‐70. - PubMed
Nickerson 2005 {published data only}
-
- Nickerson A, MacKinnon NJ, Roberts N, Saulnier L. Drug‐therapy problems, inconsistencies and omissions identified during a medication reconciliation and seamless care service. Healthcare Quarterly (Toronto, Ont.) 2005;8:65‐72. - PubMed
Pevnick 2018 {published data only}
Schnipper 2006 {published data only}
-
- Schnipper JL, Kirwin JL, Cotugno MC, Wahlstrom SA, Brown BA, Tarvin E, et al. Role of pharmacist counselling in preventing adverse drug events after hospitalisation. Archives of Internal Medicine 2006;166(5):565‐71. - PubMed
Schnipper 2011 {published data only}
-
- Schnipper JL, Liang CL, Hamann C, Karson AS, Lee J, Burdick E, et al. Effects of an electronic post‐discharge medication reconciliation tool on the 3 accuracy of ambulatory medication documentation. Journal of General Internal Medicine 2011;26(1):S324.
Tompson 2012 {published data only}
-
- Tompson AJ, Peterson GM, Jackson SL, Hughes JD, Raymond K. Utilizing community pharmacy dispensing records to disclose errors in hospital admission drug charts. International Journal of Clinical Pharmacology and Therapeutics 2012;50(9):639‐46. - PubMed
Vega 2016 {published data only}
Yau 2008 {unpublished data only}
-
- Yau P. The impact of pharmacist discharge medication reconciliation on unintentional medication discrepancies from inpatient discharges at the Alberta Cancer Board Cross Cancer Institute.. National Oncology Pharmacy Symposium 2008 New Frontiers in Oncology Pharmacy. 2008 Oct 17‐19; Calgary, Alberta.. http://www.capho.org/sites/default/files/resources/NOPS08%20Onsite%20pro... Canadian Association of Pharmacy in Oncology, 2008:154.
References to studies excluded from this review
Corbett 2011 {published data only}
-
- Corbett C, Setter S. A health IT intervention to reduce transition‐related medication discrepancies. Western Institute of Nursing Annual Communicating Nursing Research Conference. Transitions: Unifying Practice, Education, and Research to Improve Health. 2012 Jan 21; Honolulu, Hawaii. https://www.researchgate.net/publication/268146402_A_HEALTH_IT_INTERVENT... Western Institute of Nursing, 2012:269.
Fernandes 2011 {published data only}
-
- Fernandes O, Etchells E, Lee AW, Siu V, Bell C, Wong G, et al. What is the impact of a centralized provincial drug profile viewer on the quality and efficiency of patient admission medication reconciliation? A randomised controlled trial. Canadian Journal of Hospital Pharmacy 2011;64(1):85.
NCT01819974 {published data only}
-
- NCT01819974. Effect of medication reviews performed in high risk patients. clinicaltrials.gov/show/NCT1819974 (first received March 28, 2013).
NCT02047448 {published data only}
-
- NCT02047448. Improving medication adherence through a transitional care pharmacy practice model. clinicaltrials.gov/show/NCT02047448 (first received January 28, 2014).
NCT02368548 {published data only}
-
- NCT02368548. Randomized clinical trial of a pharmaceutical care program in chronic patients users of an emergency department. clinicaltrials.gov/show/NCT02368548 (first received February 23, 2015).
Quach 2015 {published data only}
-
- Quach J, Hua S, Traylor B, Burton J. Reduce medication errors by doing early medication reconciliation in the emergency department. Pharmacotherapy 2015;35:e197.
Romero 2015 {published data only}
-
- Romero CP, Hernanz BC, Fragoso AS, Gonzalez RJ, Javato MAB, Hernandez MAC. Efficacy of a reconciliation intervention by a specialized pharmacist to resolve medication‐related problems of elderly patients admitted to an emergency department short‐stay unit: a randomized clinical trial. Emergencias 2015;27:364‐70. - PubMed
References to ongoing studies
ISRCTN23949491 {published data only}
-
- ISRCTN23949491. Medicines reconciliation at the interface: a pilot randomised controlled trial to determine the costs and effects of a pharmacy provided service. www.isrctn.com/ISRCTN23949491 (first received September 9, 2012).
NCT00844025 {published data only}
-
- NCT00844025. Pharmaceutical care and clinical outcomes for the elderly taking potentially inappropriate medication: a randomized‐controlled trial. clinicaltrials.gov/show/NCT00844025 (first received February 13, 2009).
NCT01082978 {published data only}
-
- NCT01082978. Portable health files improve quality of care and health outcomes: a randomized controlled trial. clinicaltrials.gov/show/NCT01082978 (first received March 9, 2010).
NCT01195051 {published data only}
-
- NCT01195051. Medication reconciliation to improve quality of transitional care. clinicaltrials.gov/show/NCT01195051 (first received September 3, 2010).
NCT02006797 {published data only}
-
- NCT02006797. Communication between hospital and community pharmacists: impact on drug management at discharge (REPHVIM). clinicaltrials.gov/show/NCT02006797. Pourrat,Xavier. Pharmacy Department, Pharm D, Tours University Hospital, 2 boulevard Tonnelle, 37044 Tours cedex 09, France. x.pourrat@chu‐tours.fr, (first received December 10, 2013).
NCT02135731 {published data only}
-
- Lesselroth BJ, Dorr DA, Adams K, Church V, Adams S, Mazur D, et al. Medication review software to improve the accuracy of outpatient medication histories: protocol for a randomised controlled trial. Human Factors and Ergonomics in Manufacturing 2012; Vol. 22, issue 1:72‐86.
NCT02413957 {published data only}
-
- NCT02413957. Medication reconciliation in comparison to an extensive medication safety check. clinicaltrials.gov/show/NCT02413957 (first received April 10, 2015).
NCT02482025 {published data only}
-
- NCT02482025. The Secure Messaging for Medication Reconciliation Tool (SMMRT) trial. clinicaltrials.gov/show/NCT02482025 (first received June 25, 2015).
NCT02598115 {published data only}
-
- NCT02598115. Impact of collaborative pharmaceutical care on hospital admission drug prescriptions for patients 65 years of age and older (MEDREV). clinicaltrials.gov/ct2/show/NCT02598115 (first received November 5, 2015).
NCT02689076 {published data only}
-
- NCT02689076. Regional data exchange to improve care for Veterans after non‐VA hospitalization. clinicaltrials.gov/ct2/show/NCT02689076 (first received February 23, 2016).
NCT02871115 {published data only}
-
- NCT02871115. Pilot study of a pharmacy intervention for older adults with cancer. clinicaltrials.gov/ct2/show/NCT02871115 (first received August 18, 2016).
NCT02905474 {published data only}
-
- NCT02905474. Mobile health technology for chronic kidney disease patients: medication management. clinicaltrials.gov/ct2/show/NCT02905474 (first received September 19, 2016).
NCT03029052 {published data only}
-
- NCT03029052. Medication reconciliation at discharge: impact on patient's care (CONCIVILLE). clinicaltrials.gov/ct2/show/NCT03029052 (first received January 24, 2017).
NCT03173690 {published data only}
-
- NCT03173690. Medicines reconciliation at an intensive care unit. clinicaltrials.gov/ct2/show/NCT03173690 (first received June 2, 2017).
Westbrook 2016 {published data only}
-
- Westbrook JI, Li L, Raban MZ, Baysari MT, Mumford V, Prgomet M, et al. Stepped‐wedge cluster randomised controlled trial to assess the effectiveness of an electronic medication management system to reduce medication errors, adverse drug events and average length of stay at two paediatric hospitals: a study protocol. BMJ Open 2016;6:e011811. - PMC - PubMed
Williams 2013 {published data only}
-
- Williams M, Swearingen K, Cavanaugh T. Project impact: improving patient adherence through communication at transition. Journal of the American Pharmacists Association 2013;53:e16.
Additional references
Bassi 2010
-
- Bassi Jesdeep, Lau Francis, Bardal Stan. Use of Information Technology in Medication Reconciliation: A Scoping Review. Annals of Pharmacotherapy (USA) 2010;44(5):885‐97. - PubMed
Bates 1995
-
- Bates DW, Cullen DJ, Laird N, Petersen LA, Small SD, Servi D, et al. Incidence of adverse drug events and potential adverse drug events. Implications for prevention. ADE Prevention Study Group. JAMA 1995;274(1):29‐34. - PubMed
Bates 2007
-
- Bates DW. Preventing medication errors: a summary. American Journal of Health‐system Pharmacy 2007;64(14 Suppl 9):S3‐9. - PubMed
Bayoumi 2009
-
- Bayoumi Imaan, Howard Michelle, Holbrook Anne M, Schabort Inge. Interventions to improve medication reconciliation in primary care. The Annals of pharmacotherapy 2009;43(10):1667‐75. - PubMed
Boockvar 2006
-
- Boockvar KS, Carlson LaCorte H, Giambanco V, Fridman B, Siu A. Medication reconciliation for reducing drug‐discrepancy adverse events. American Journal of Geriatric Pharmacotherapy 2006;4(3):236‐43. - PubMed
Carter 2008
Chhabra 2012
-
- Chhabra Pankdeep T, Rattinger Gail B, Dutcher Sarah K, Hare Melanie E, Parsons Kelly L, Zuckerman Ilene H. Medication reconciliation during the transition to and from long‐term care settings: a systematic review. Research in social & administrative pharmacy : RSAP 2012;8(1):60‐75. - PubMed
Coleman 2003a
-
- Coleman EA, Boult C. Improving the quality of transitional care for persons with complex care needs. Journal of the American Geriatrics Society 2003;51(4):556‐7. - PubMed
Coleman 2003b
-
- Coleman EA. Falling through the cracks: challenges and opportunities for improving transitional care for persons with continuous complex care needs. Journal of the American Geriatrics Society 2003;51(4):549‐55. - PubMed
Coleman 2004
-
- Coleman EA, Berenson RA. Lost in transition: challenges and opportunities for improving the quality of transitional care. Annals of Internal Medicine 2004;141(7):533‐6. - PubMed
Cornish 2005
-
- Cornish PL, Knowles SR, Marchesano R, Tam V, Shadowitz S, Juurlink DN, et al. Unintended medication discrepancies at the time of hospital admission. Archives of Internal Medicine 2005;165(4):424‐9. [PUBMED: 15738372] - PubMed
Donaldson 2017
-
- Donaldson LJ, Kelley ET, Dhingra‐Kumar N, Kieny MP, Sheikh A. Medication without harm: WHO's third global patient safety challenge. Lancet 2017;389(10080):1680‐1. - PubMed
EPOC 2013a
-
- Cochrane Effective Practice and Organisation of Care (EPOC) Group. Effective Practice and Organisation of Care (EPOC). EPOC taxonomy; 2013. epoc.cochrane.org/epoc‐taxonomy (accessed 17 October 2013).
EPOC 2013b
-
- Cochrane Effective Practice and Organisation of Care (EPOC) Group. What outcomes should be reported in EPOC reviews? EPOC Resources for review authors, 2017. epoc.cochrane.org/resources/epoc‐resources‐review‐authors (accessed 17 October 2013).
EPOC 2013c
-
- Cochrane Effective Practice and Organisation of Care (EPOC) Group. Cochrane Effective Practice and Organisation of Care (EPOC). Data collection form. EPOC Resources for review authors, 2017. epoc.cochrane.org/epoc‐specific‐resources‐review‐authors (accessed 17 October 2013).
Forster 2003
-
- Forster AJ, Murff HJ, Peterson JF, Gandhi TK, Bates DW. The incidence and severity of adverse events affecting patients after discharge from the hospital. Annals of Internal Medicine 2003;138(3):161‐7. - PubMed
Gillespie 2009
-
- Gillespie U, Alassaad A, Henrohn D, Garmo H, Hammarlund‐Udenaes M, Toss H, et al. A comprehensive pharmacist intervention to reduce morbidity in patients 80 years or older: a randomised controlled trial. Archives of Internal Medicine 2009;169(9):894‐900. - PubMed
GRADEpro GDT 2015 [Computer program]
-
- McMaster University (developed by Evidence Prime, Inc.). GRADEpro Guideline Development Tool. Hamilton (ON): McMaster University (developed by Evidence Prime, Inc.), 2015.
Greenwald 2010
-
- Greenwald JL, Halasyamani L, Greene J, LaCivita C, Stucky E, Benjamin B, et al. Making inpatient medication reconciliation patient entered, clinically relevant and implementable: a consensus statement on key principles and necessary first steps. Journal of Hospital Medicine 2010;5(8):477‐85. - PubMed
Higgins 2011
-
- Higgins JP, Green S, editor(s). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 (updated March 2011). The Cochrane Collaboration, 2011. Available from handbook.cochrane.org.
Hughes 2008
-
- Hughes RG, editor. Patient safety and quality: an evidence‐based handbook for nurses. (Prepared with support from the Robert Wood Johnson Foundation.) AHRQ Publication No. 08‐0043. Rockville, MD: Agency for Healthcare Research and Quality; March 2008. www.ahrq.gov/professionals/clinicians‐providers/resources/nursing/resour... (accessed 17 October 2013). - PubMed
IHI 2011
-
- Institute for Healthcare Improvement. How‐to guide: prevent adverse drug events by implementing medication reconciliation. www.ihi.org/_layouts/ihi/login/login.aspx?ReturnURL=%2fknowledge%2fPages... (accessed 17 October 2013).
Karapinar 2011
-
- Karapinar F, Terry DR. Medication reconciliation : a necessity for continuity of care (EAHP 16th Congress Report). European Journal of Hospital Pharmacy: Practice 2011;17:32‐3.
Karnon 2009
-
- Karnon Jonathan, Campbell Fiona, Czoski‐Murray Carolyn. Model‐based cost‐effectiveness analysis of interventions aimed at preventing medication error at hospital admission (medicines reconciliation). Journal of Evaluation in Clinical Practice 2009;15(2):299‐306. - PubMed
Kim 2013
-
- Kim CS, Flanders SA. Transitions of care. Annals of Internal Medicine 2013;158(5 Pt 1):ITC3‐1. - PubMed
Koehler 2009
-
- Koehler BE, Richter KM, Youngblood L, Cohen BA, Prengler ID, Cheng D, et al. Reduction of 30‐day postdischarge hospital readmission or emergency department (ED) visit rates in high‐risk elderly medical patients through delivery of a targeted care bundle. Journal of Hospital Medicine 2009;4(4):211‐8. - PubMed
Kramer 2007
-
- Kramer JS, Hopkins PJ, Rosendale JC, Garrelts JC, Hale LS, Nester TM, et al. Implementation of an electronic system for medication reconciliation. American Journal of Health‐system Pharmacy 2007;64(4):404‐22. - PubMed
Kwan 2013
-
- Kwan JL, Lo L, Sampson M, Shojania KG. Medication reconciliation during transitions of care as a patient safety strategy: a systematic review. Annals of Internal Medicine 2013;158(5 Pt 2):397‐403. - PubMed
Lehnbom 2014
-
- Lehnbom Elin C, Stewart Michael J, Manias Elizabeth, Westbrook Johanna I. Impact of medication reconciliation and review on clinical outcomes. The Annals of pharmacotherapy 2014;48(10):1298‐312. - PubMed
Mekonnen 2016
-
- Mekonnen Alemayehu B, McLachlan Andrew J, Brien Jo‐anne E. Pharmacy‐led medication reconciliation programmes at hospital transitions: a systematic review and meta‐analysis. Journal of clinical pharmacy and therapeutics 2016;41(2):128‐44. - PubMed
Mekonnen 2016a
Moore 2003
Mueller 2012
Naranjo 1992
-
- Naranjo CA, Shear NH, Lanctôt KL. Advances in the diagnosis of adverse drug reactions. Journal of Clinical Pharmacology 1992;32(10):897‐904. - PubMed
Nazar 2015
NICE 2007
-
- National Institute for Health and Care Excellence. Technical patient safety solutions for medicines reconciliation on admission of adults to hospital: guidance. guidance.nice.org.uk/PSG001 (accessed prior to 17 July 2018).
Review Manager 2013 [Computer program]
-
- The Nordic Cochrane Centre, The Cochrane Collaboration. Review Manager (RevMan). Version 5.2. Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2013.
Schnipper 2009
-
- Schnipper JL, Hamann C, Ndumele CD, Liang CL, Carty MG, Karson AS, et al. Effect of an electronic medication reconciliation application and process redesign on potential adverse drug events: a cluster‐randomised trial. Archives of Internal Medicine 2009;169(8):771‐80. - PubMed
Schünemann 2013
-
- Schünemann H, Brozek J, Guyatt G, Oxman AD, editors. GRADE Handbook for Grading Quality of Evidence and Strength of Recommendations. GRADE Working Group, 2013.
Spinewine 2013
-
- Spinewine Anne, Claeys Coraline, Foulon Veerle, Chevalier Pierre. Approaches for improving continuity of care in medication management: a systematic review. International journal for quality in health care 2013;25(4):403‐17. - PubMed
Strand 1990
-
- Strand L M, Morley P C, Cipolle R J, Ramsey R, Lamsam G D. Drug‐related problems: their structure and function. DICP : the annals of pharmacotherapy 1990;24(11):1093‐7. - PubMed
Tam 2005
The Joint Commission 2013
-
- The Joint Commission. National Patient Safety Goals. www.jointcommission.org/standards_information/npsgs.aspx (accessed 17 October 2013).
WHO 2006
-
- World Health Organization. Action on Patient Safety – High 5s. http://www.who.int/patientsafety/topics/high‐5s/en/ (accessed 5 August 2018).
References to other published versions of this review
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical