

Lower Pretreatment Gut Integrity Is Independently Associated With Fat Gain on Antiretroviral Therapy
- PMID: 30137242
- PMCID: PMC6599164
- DOI: 10.1093/cid/ciy716
Lower Pretreatment Gut Integrity Is Independently Associated With Fat Gain on Antiretroviral Therapy
Abstract
Background: Fat accumulation and insulin resistance remain a threat to the success of antiretroviral therapy (ART). The role of gut dysfunction in metabolic complications associated with ART initiation is unclear.
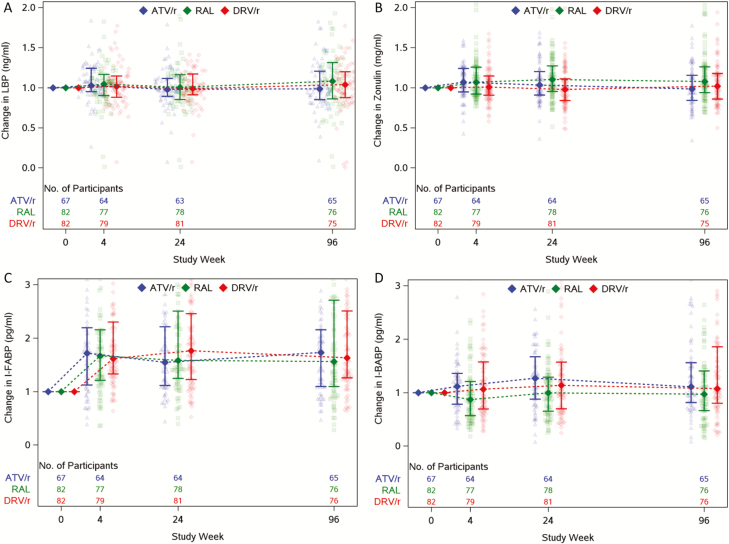
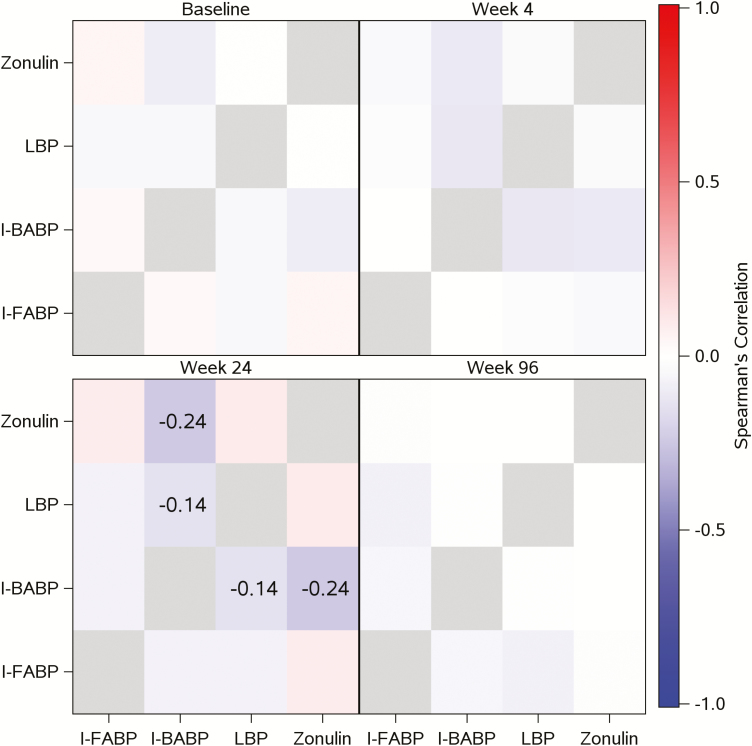
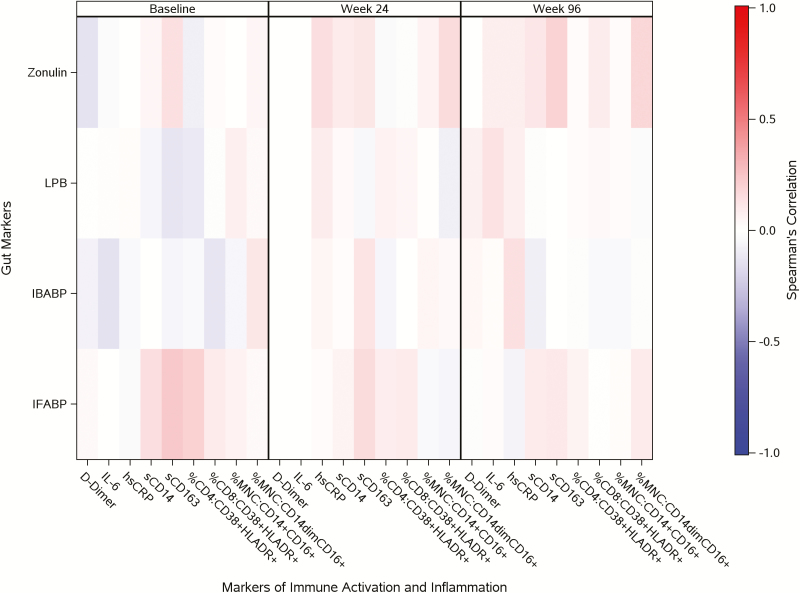
Methods: Human immunodeficiency virus (HIV)-infected ART-naive participants were randomized to tenofovir disoproxil fumarate/emtricitabine plus atazanavir/ritonavir, darunavir/ritonavir, or raltegravir (RAL). Changes in the gut integrity markers zonulin, lipopolysaccharide-binding protein (LBP), and intestinal fatty acid and ileal bile acid binding proteins (I-FABP and I-BABP) were assessed over 96 weeks. Wilcoxon rank-sum tests were used to compare changes between groups and linear regression models to quantify associations between gut markers, insulin resistance, body mass index (BMI), and visceral, subcutaneous, and total adipose tissue (VAT, SAT, and TAT).
Results: : 90% were male and 48% were White non-Hispanic. The median age was 36 years, HIV-1 ribonucleic acid was 4.56 log10 copies/mL, and CD4 count was 338 cells/µL. An overall 1.7-fold increase in I-FABP was observed throughout 96 weeks, with no difference between arms. Zonulin levels increased with RAL compared to protease inhibitor-based regimens (week 96, P = .02); minimal changes in I-BABP or LBP levels were observed. Higher baseline I-FABP levels were associated with increases in VAT, TAT, and BMI (16%, 9%, and 2.5%, respectively; P < .04) over 96 weeks.
Conclusions: While ART induces changes in the markers of gut barrier dysfunction, the extent to which they improve or worsen the gut barrier function remains unclear. Nevertheless, markers of gut barrier dysfunction in ART-naive individuals predict increases in total and visceral abdominal fat with treatment initiation.
Keywords: body composition; gut integrity; microbial translocation.
© The Author(s) 2018. Published by Oxford University Press for the Infectious Diseases Society of America. All rights reserved. For permissions, e-mail: journals.permissions@oup.com.
Figures
Similar articles
-
Body Composition Changes After Initiation of Raltegravir or Protease Inhibitors: ACTG A5260s.Clin Infect Dis. 2016 Apr 1;62(7):853-62. doi: 10.1093/cid/ciw017. Epub 2016 Jan 20. Clin Infect Dis. 2016. PMID: 26797215 Free PMC article. Clinical Trial.
-
Changes in Bone Mineral Density After Initiation of Antiretroviral Treatment With Tenofovir Disoproxil Fumarate/Emtricitabine Plus Atazanavir/Ritonavir, Darunavir/Ritonavir, or Raltegravir.J Infect Dis. 2015 Oct 15;212(8):1241-9. doi: 10.1093/infdis/jiv194. Epub 2015 May 5. J Infect Dis. 2015. PMID: 25948863 Free PMC article. Clinical Trial.
-
Antiretroviral Therapy Initiation Is Associated With Decreased Visceral and Subcutaneous Adipose Tissue Density in People Living With Human Immunodeficiency Virus.Clin Infect Dis. 2021 Mar 15;72(6):979-986. doi: 10.1093/cid/ciaa196. Clin Infect Dis. 2021. PMID: 32107532 Free PMC article. Clinical Trial.
-
Differential body composition effects of protease inhibitors recommended for initial treatment of HIV infection: a randomized clinical trial.Clin Infect Dis. 2015 Mar 1;60(5):811-20. doi: 10.1093/cid/ciu898. Epub 2014 Nov 10. Clin Infect Dis. 2015. PMID: 25389256 Clinical Trial.
-
The impact of HIV antiretroviral therapy on gut microbiota: the need for well-designed longitudinal studies.J Infect Dev Ctries. 2024 Oct 31;18(10):1461-1473. doi: 10.3855/jidc.18878. J Infect Dev Ctries. 2024. PMID: 39616473 Free PMC article. Review.
Cited by
-
Insulin resistance and intestinal integrity in children with and without HIV infection in Uganda.HIV Med. 2020 Feb;21(2):119-127. doi: 10.1111/hiv.12808. Epub 2019 Oct 23. HIV Med. 2020. PMID: 31642582 Free PMC article.
-
Cardiometabolic Complications in Youth With Perinatally Acquired HIV in the Era of Antiretroviral Therapy.Curr HIV/AIDS Rep. 2021 Oct;18(5):424-435. doi: 10.1007/s11904-021-00574-x. Epub 2021 Oct 15. Curr HIV/AIDS Rep. 2021. PMID: 34652624 Free PMC article. Review.
-
Effects of different integrase strand transfer inhibitors on body weight in patients with HIV/AIDS: a network meta-analysis.BMC Infect Dis. 2022 Feb 3;22(1):118. doi: 10.1186/s12879-022-07091-1. BMC Infect Dis. 2022. PMID: 35114968 Free PMC article.
-
Mapping the Gut Microbiota Composition in the Context of Raltegravir, Dolutegravir, and Bictegravir-A Scoping Review.Int J Mol Sci. 2025 Jul 2;26(13):6366. doi: 10.3390/ijms26136366. Int J Mol Sci. 2025. PMID: 40650144 Free PMC article.
-
Association Between Body Mass Index Variation and Early Mortality Among 834 Ethiopian Adults Living with HIV on ART: A Joint Modelling Approach.Infect Dis Ther. 2023 Jan;12(1):227-244. doi: 10.1007/s40121-022-00726-5. Epub 2022 Nov 28. Infect Dis Ther. 2023. PMID: 36443546 Free PMC article.
References
-
- Guaraldi G, Luzi K, Bellistrì GM, et al. . CD8 T-cell activation is associated with lipodystrophy and visceral fat accumulation in antiretroviral therapy-treated virologically suppressed HIV-infected patients. J Acquir Immune Defic Syndr 2013; 64:360–6. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
