

Single vs. dual chamber implantable cardioverter-defibrillators or programming of implantable cardioverter-defibrillators in patients without a bradycardia pacing indication: systematic review and meta-analysis
- PMID: 30137296
- PMCID: PMC6182310
- DOI: 10.1093/europace/euy183
Single vs. dual chamber implantable cardioverter-defibrillators or programming of implantable cardioverter-defibrillators in patients without a bradycardia pacing indication: systematic review and meta-analysis
Abstract
Aims: Implantable cardioverter-defibrillators (ICDs) are key in the prevention of sudden cardiac death, but outcomes may vary by type of device or programming [single chamber (SC) vs. dual chamber (DC)] in patients without a bradycardia pacing indication. We sought to meta-analyse patient outcomes of randomized trials of SC vs. DC devices or programming.
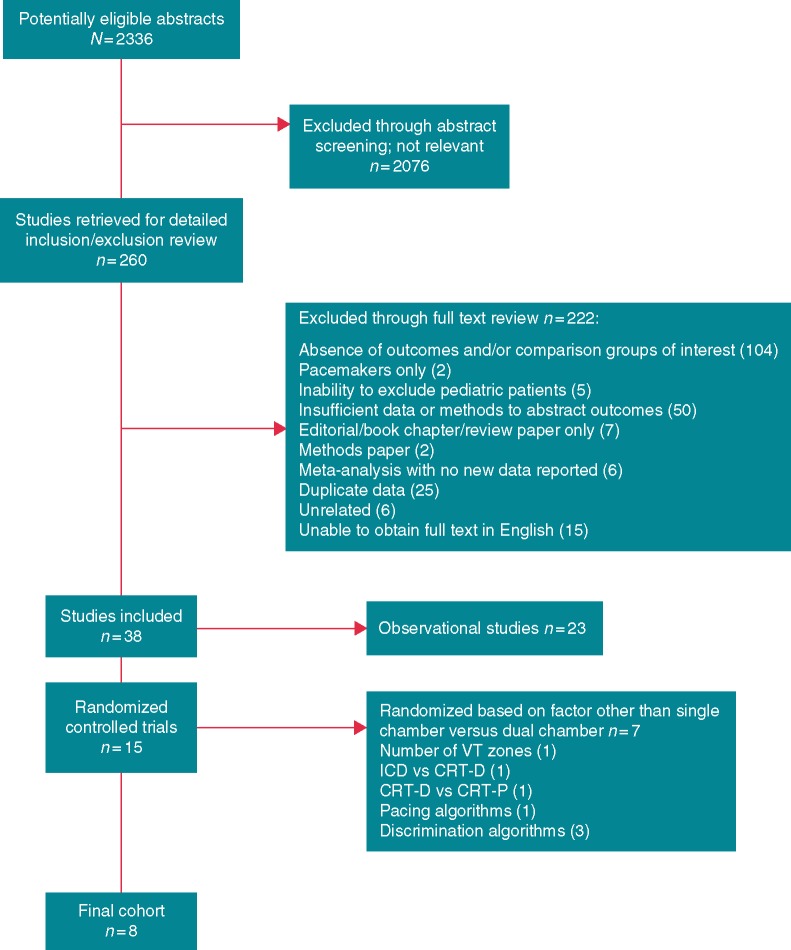
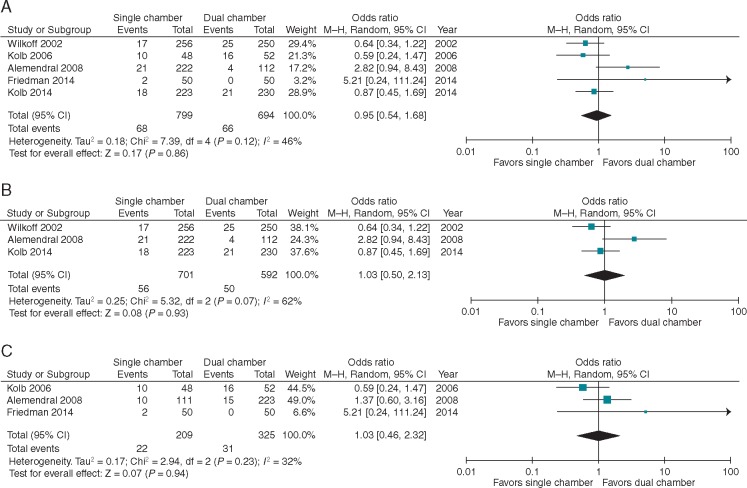
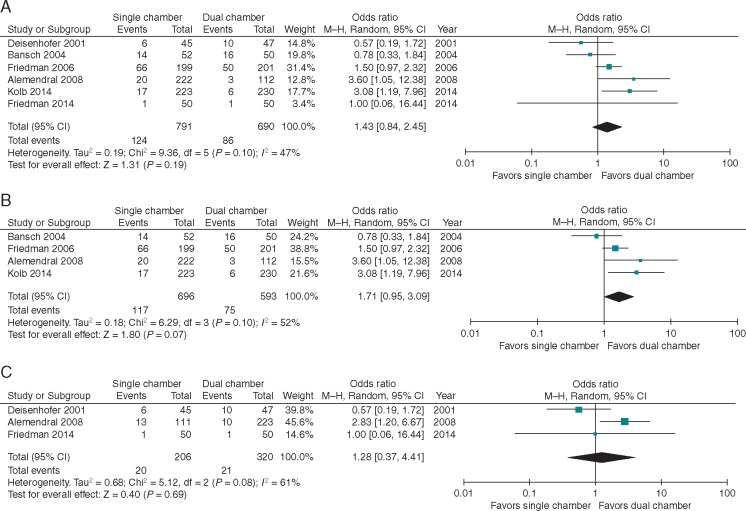
Methods and results: We searched PubMed, Embase, Scopus, Web of Science, and Cochrane trials databases for relevant studies excluding those published before 2000, involving children, or not available in English. Endpoints included mortality, inappropriate ICD therapies, and implant complications. Endpoints with at least three reporting studies were meta-analysed. We identified eight studies meeting inclusion criteria representing 2087 patients with 16.1 months mean follow-up. Mean age was 62.7 years (SD 1.92); in six studies reporting sex, most patients were male (85%). Comparing patients with a SC or DC ICD or programming, we found similar rates of mortality [odds ratio (OR) 0.95, 95% confidence interval (CI) 0.54-1.68; P = 0.86] and inappropriate therapies (OR 1.46, 95% CI 0.97-2.19; P = 0.07) in five and six studies, respectively. In three studies of SC vs. DC ICDs (but not programming) rates of pneumothorax and lead dislodgement were not different (OR 2.12, 95% CI 0.18-24.72; P = 0.55 and OR 0.87, 95% CI 0.32-2.47; P = 0.83, respectively).
Conclusion: In this meta-analysis of randomized controlled trials comparing SC vs. DC ICD device or programming, there was no significant difference in inappropriate therapies, mortality, pneumothorax, or lead dislodgement. Future studies should compare these devices over longer follow-up and in specific patient populations.
Figures


Similar articles
-
Efficiencies and Complications of Dual Chamber versus Single Chamber Implantable Cardioverter Defibrillators in Secondary Sudden Cardiac Death Prevention: A Meta-analysis.Heart Lung Circ. 2016 Feb;25(2):148-54. doi: 10.1016/j.hlc.2015.07.008. Epub 2015 Aug 10. Heart Lung Circ. 2016. PMID: 26338316 Review.
-
Comparison of Inappropriate Shocks and Other Health Outcomes Between Single- and Dual-Chamber Implantable Cardioverter-Defibrillators for Primary Prevention of Sudden Cardiac Death: Results From the Cardiovascular Research Network Longitudinal Study of Implantable Cardioverter-Defibrillators.J Am Heart Assoc. 2017 Nov 9;6(11):e006937. doi: 10.1161/JAHA.117.006937. J Am Heart Assoc. 2017. PMID: 29122811 Free PMC article.
-
Dual- vs. single-chamber defibrillators for primary prevention of sudden cardiac death: long-term follow-up of the Défibrillateur Automatique Implantable-Prévention Primaire registry.Europace. 2017 Sep 1;19(9):1478-1484. doi: 10.1093/europace/euw230. Europace. 2017. PMID: 28340096
-
A prospective randomized trial of single- or dual-chamber implantable cardioverter-defibrillators to minimize inappropriate shock risk in primary sudden cardiac death prevention.Europace. 2014 Oct;16(10):1460-8. doi: 10.1093/europace/euu022. Epub 2014 Jun 13. Europace. 2014. PMID: 24928948 Clinical Trial.
-
The subcutaneous implantable cardioverter-defibrillator in review.Am Heart J. 2019 Nov;217:131-139. doi: 10.1016/j.ahj.2019.08.010. Epub 2019 Aug 17. Am Heart J. 2019. PMID: 31654943 Review.
Cited by
-
Major gaps in the information provided to patients before implantation of cardioverter defibrillators: a prospective patient European evaluation.Europace. 2023 Mar 30;25(3):1144-1151. doi: 10.1093/europace/euac275. Europace. 2023. Retraction in: Eur J Heart Fail. 2022 Aug;24(8):1454. doi: 10.1002/ejhf.2600. PMID: 36691111 Free PMC article. Retracted.
-
How to get the optimal defibrillation lead parameters using myocardial perfusion scintigraphy in patients with coronary artery disease.Int J Cardiovasc Imaging. 2021 Nov;37(11):3323-3333. doi: 10.1007/s10554-021-02308-x. Epub 2021 Jun 7. Int J Cardiovasc Imaging. 2021. PMID: 34100141
-
[History of the implantable cardioverter-defibrillator in Germany].Herzschrittmacherther Elektrophysiol. 2024 Mar;35(Suppl 1):55-67. doi: 10.1007/s00399-024-01001-5. Epub 2024 Feb 29. Herzschrittmacherther Elektrophysiol. 2024. PMID: 38421401 Free PMC article. Review. German.
-
Ability to remotely monitor atrial high-rate episodes using a single-chamber implantable cardioverter-defibrillator with a floating atrial sensing dipole.Europace. 2023 May 19;25(5):euad061. doi: 10.1093/europace/euad061. Europace. 2023. PMID: 37038759 Free PMC article.
-
Determinants of inappropriate implantable cardioverter-defibrillator shocks: the German Device Registry perspective.J Interv Card Electrophysiol. 2019 Oct;56(1):71-77. doi: 10.1007/s10840-019-00600-4. Epub 2019 Aug 2. J Interv Card Electrophysiol. 2019. PMID: 31375974
References
-
- Hallstrom AP, Greene HL, Wyse DG, Zipes D, Epstein AE, Domanski MJ. et al. Antiarrhythmics versus implantable defibrillators (AVID)—rationale, design, and methods. Am J Cardiol 1995;75:470–5. - PubMed
-
- Kuck KH, Cappato R, Siebels J, Ruppel R.. Randomized comparison of antiarrhythmic drug therapy with implantable defibrillators in patients resuscitated from cardiac arrest: the Cardiac Arrest Study Hamburg (CASH). Circulation 2000;102:748–54. - PubMed
-
- Moss AJ, Zareba W, Hall WJ, Klein H, Wilber DJ, Cannom DS. et al. Prophylactic implantation of a defibrillator in patients with myocardial infarction and reduced ejection fraction. N Engl J Med 2002;346:877–83. - PubMed
-
- Dewland TA, Pellegrini CN, Wang Y, Marcus GM, Keung E, Varosy PD.. Dual-chamber implantable cardioverter-defibrillator selection is associated with increased complication rates and mortality among patients enrolled in the NCDR implantable cardioverter-defibrillator registry. J Am Coll Cardiol 2011;58:1007–13. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
