

New insights into the timing and potential mechanisms of respiratory-induced cortical arousals in obstructive sleep apnea
- PMID: 30137568
- PMCID: PMC6231527
- DOI: 10.1093/sleep/zsy160
New insights into the timing and potential mechanisms of respiratory-induced cortical arousals in obstructive sleep apnea
Abstract
Study objectives: A negative intrathoracic pressure threshold is one commonly proposed mechanism for triggering respiratory-induced arousals in obstructive sleep apnea (OSA). If so, they should occur during inspiration, shortly after maximal negative pressure swings. Alternatively, respiratory-induced arousals may occur throughout the respiratory cycle if other mechanisms also contribute. However, arousal timing has been minimally investigated. This study aimed to (1) determine the temporal relationship between respiratory-induced arousals and breathing phase and (2) characterize neuromuscular and load compensation responses prior to arousal.
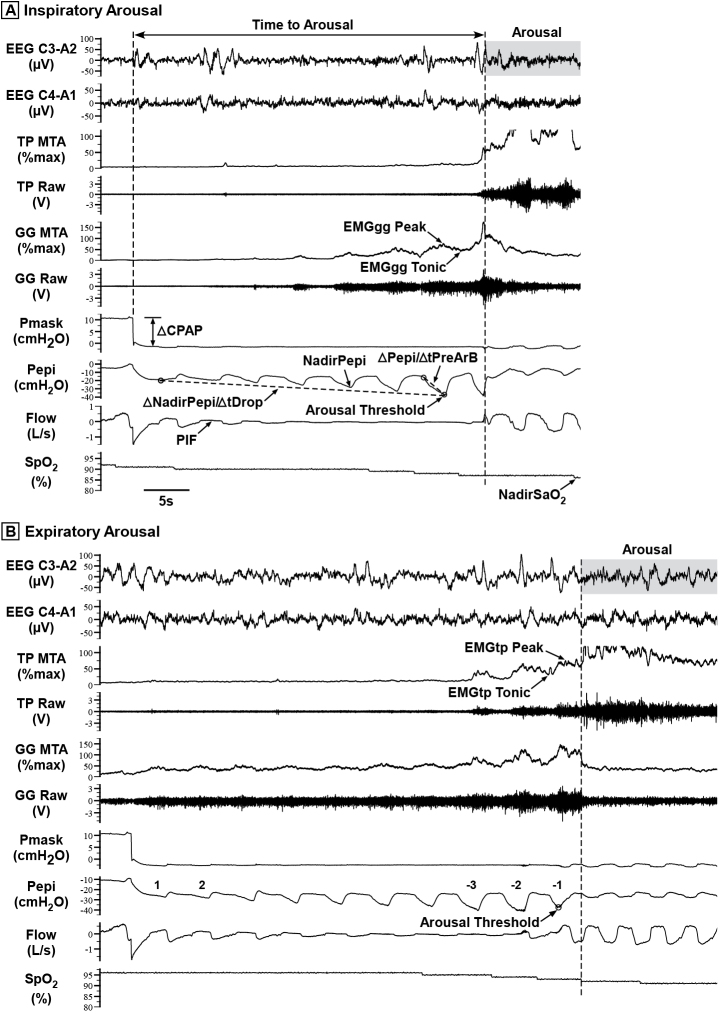
Methods: Fifty-one CPAP-treated OSA patients underwent a sleep physiology study with genioglossus and tensor palatini EMG, nasal mask/pneumotachograph, and epiglottic pressure. Transient CPAP reductions were delivered to induce respiratory-related arousals.
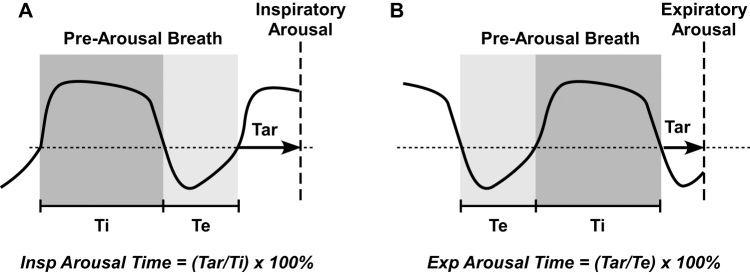
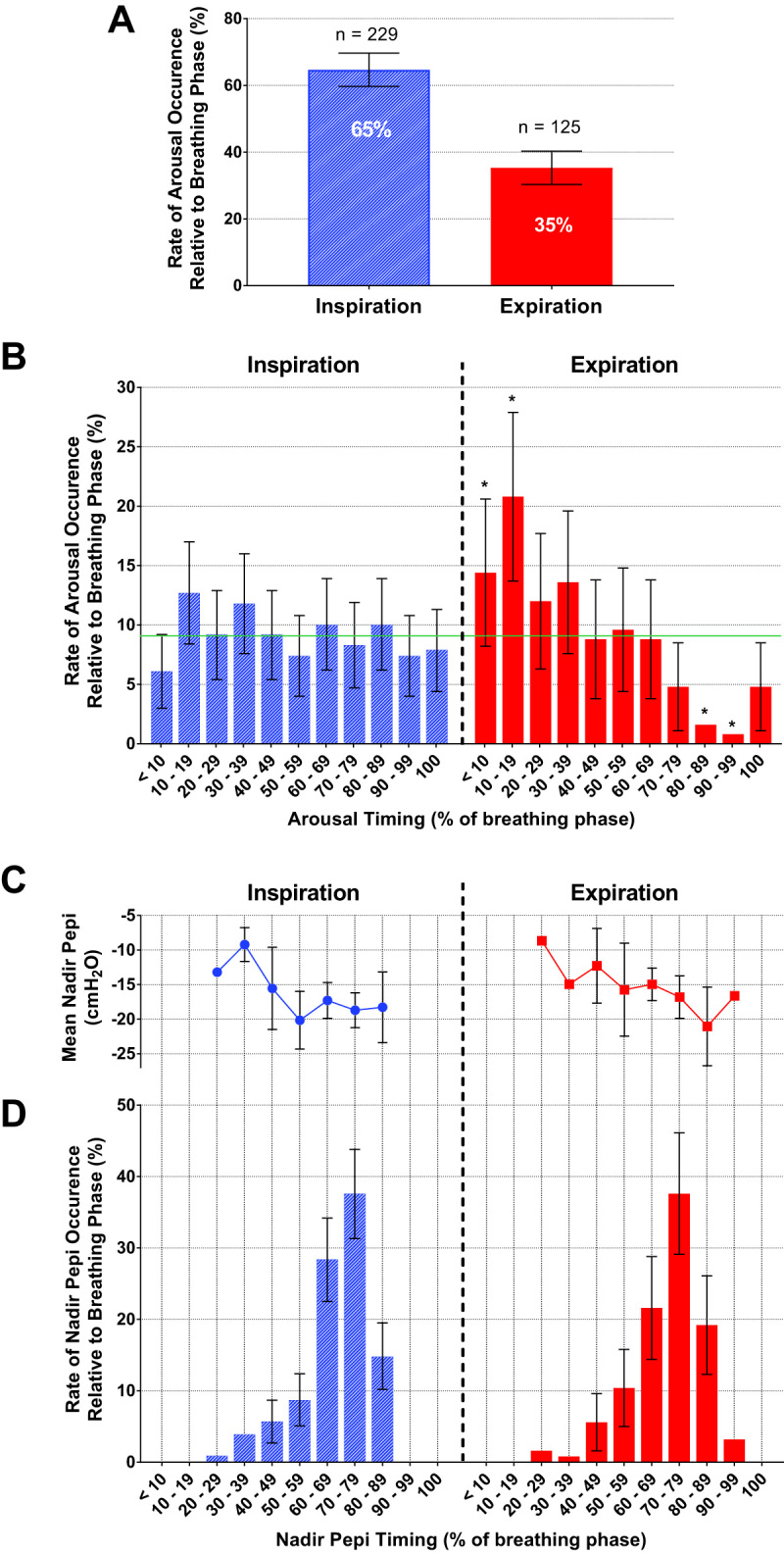
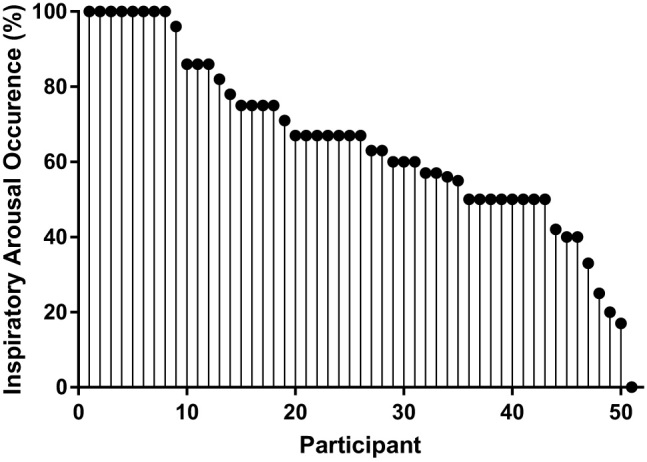
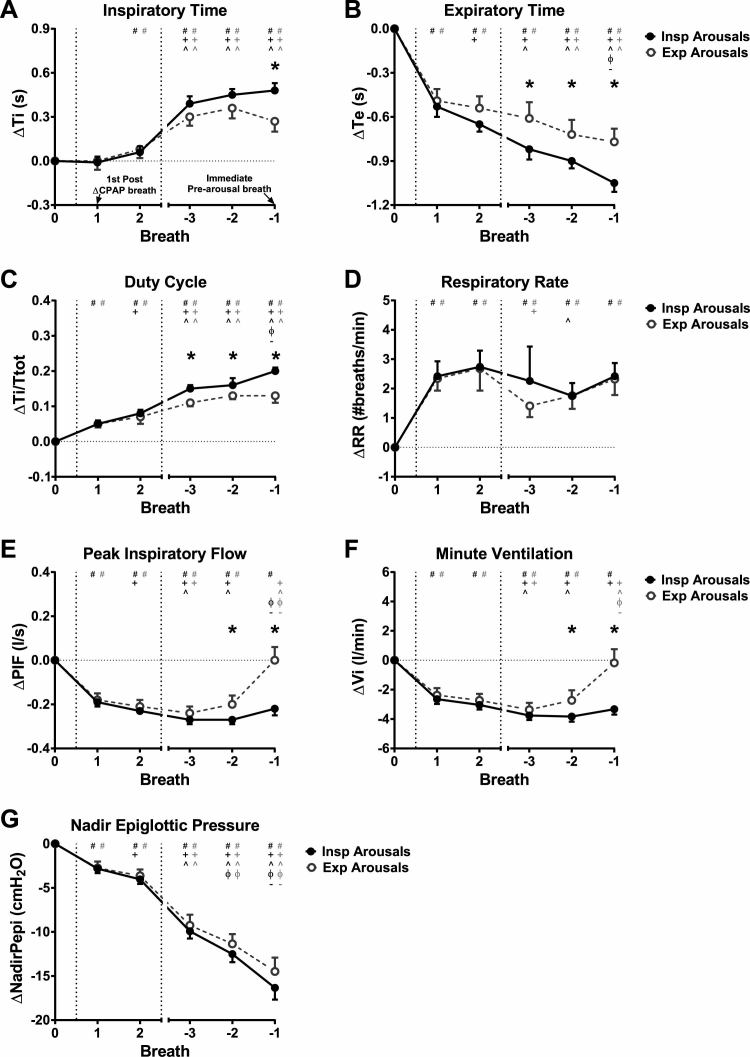
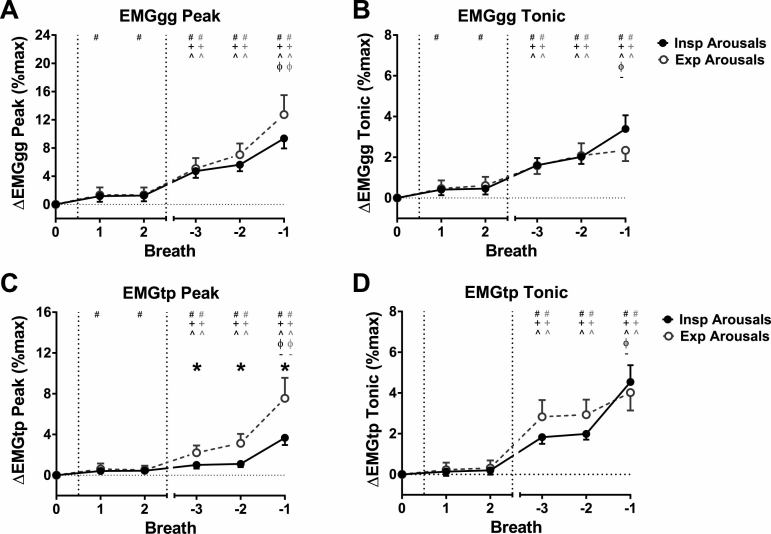
Results: Of 354 arousals, 65(60-70)%[mean(CI)] occurred during inspiration, 35(30-40)% during expiration. Nadir epiglottic pressure occurred 68(66-69)% into inspiration while inspiratory arousals had a uniform distribution throughout inspiration. Expiratory arousals occurred predominantly in early expiration. CPAP reductions initially reduced minute ventilation by ~2.5 liter/min, which was restored immediately prior to expiratory but not inspiratory arousals. Duty cycle just prior to arousal was greater for inspiratory versus expiratory arousals [0.20(0.18-0.21) vs. 0.13(0.11-0.15)Δbaseline, p = 0.001]. Peak tensor palatini EMG was higher for expiratory versus inspiratory arousals during prearousal breaths [7.6(5.8-9.6) vs. 3.7(3.0-4.5)%Δbaseline, p = 0.001], whereas genioglossus and tonic tensor palatini EMG were similar between arousal types.
Conclusions: Over one third of respiratory-induced arousals occur during expiration. These findings highlight the importance of nonpressure threshold mechanisms of respiratory-induced arousals in OSA and suggest that expiratory arousals may be a novel marker of enhanced tensor palatini neuromuscular compensation.
Figures
References
-
- Phillipson EA, et al. Arousal: the forgotten response to respiratory stimuli. Am Rev Respir Dis. 1978;118(5):807–809. - PubMed
-
- Eckert DJ, et al. Arousal from sleep: implications for obstructive sleep apnea pathogenesis and treatment. J Appl Physiol (1985). 2014;116(3):302–313. - PubMed
-
- Younes M. Role of arousals in the pathogenesis of obstructive sleep apnea. Am J Respir Crit Care Med. 2004;169(5):623–633. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
