

Glioblastoma Treated With Magnetic Resonance Imaging-Guided Laser Interstitial Thermal Therapy: Safety, Efficacy, and Outcomes
- PMID: 30137606
- PMCID: PMC6425465
- DOI: 10.1093/neuros/nyy375
Glioblastoma Treated With Magnetic Resonance Imaging-Guided Laser Interstitial Thermal Therapy: Safety, Efficacy, and Outcomes
Abstract
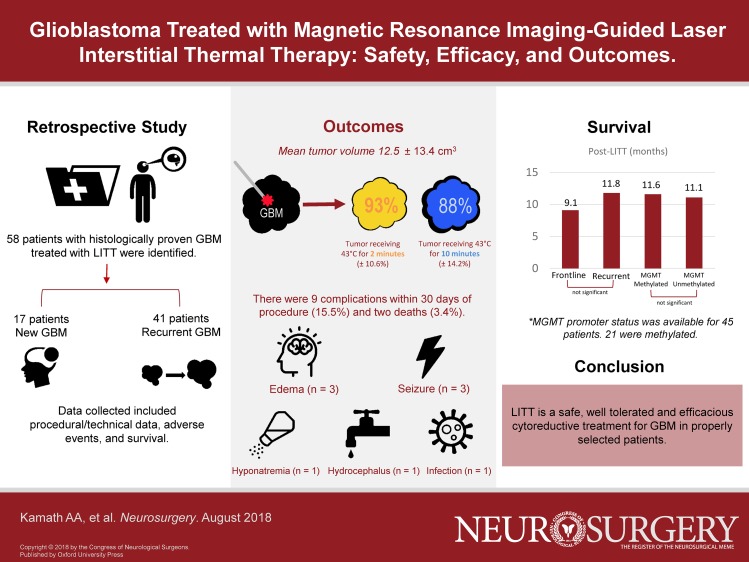
Background: Despite the multitude of available treatments, glioblastoma (GBM) remains an aggressive and uniformly fatal tumor. Laser interstitial thermal therapy (LITT) is a novel, minimally invasive treatment that holds promise for treating patients with GBM who are not candidates for traditional open craniotomy. However, due to the recent introduction of LITT into clinical practice, large series that evaluate safety and long-term outcomes after LITT are lacking.
Objective: To present our institution's series of over 50 GBM patients treated with LITT, with regard to safety, efficacy, and outcomes.
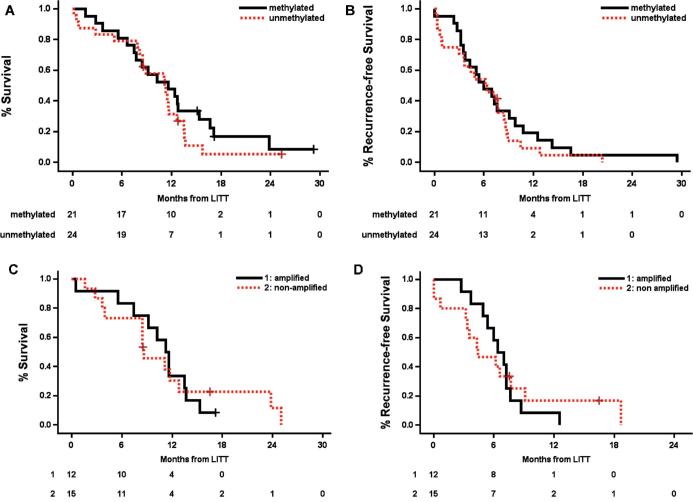
Methods: We performed a retrospective descriptive study of patients with histologically proven GBM who underwent LITT. Data collected included demographics, tumor location and volume, tumor genetic markers, treatment volume, perioperative complications, and long-term follow-up data.
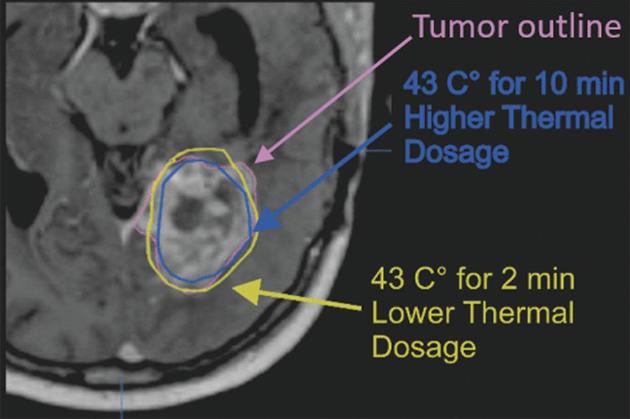
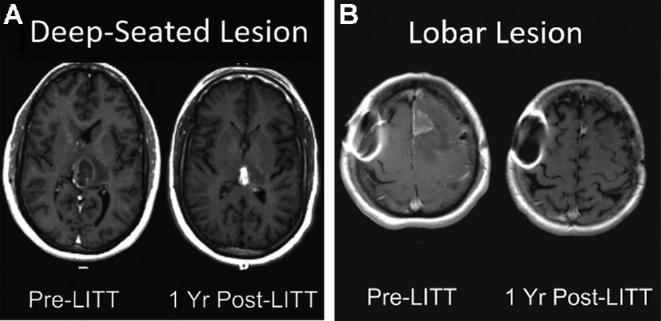
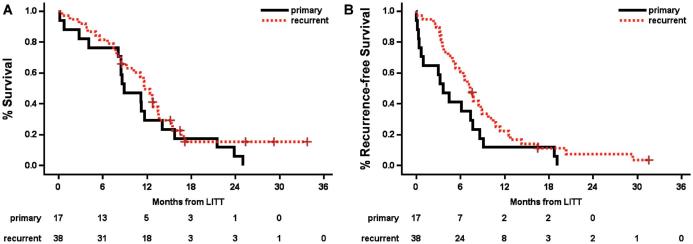
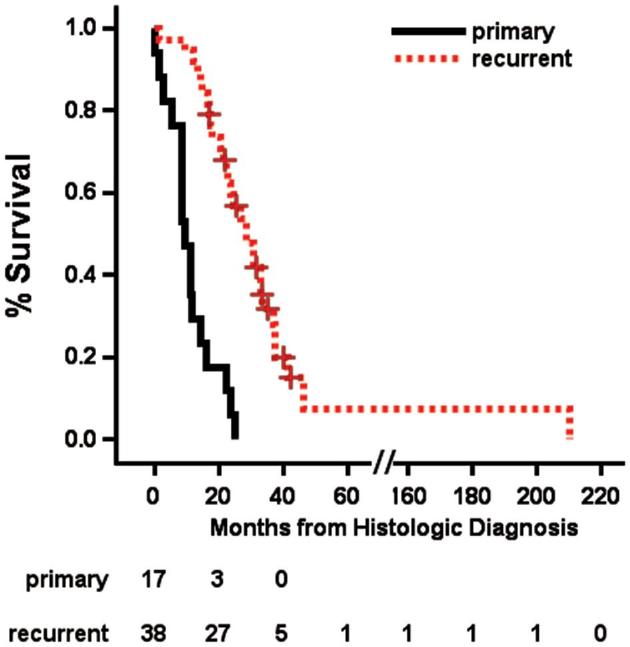
Results: We performed 58 LITT treatments for GBM in 54 patients over 5.5 yr. Forty-one were recurrent tumors while 17 were frontline treatments. Forty GBMs were lobar in location, while 18 were in deep structures (thalamus, insula, corpus callosum). Average tumor volume was 12.5 ± 13.4 cm3. Average percentage of tumor treated with the yellow thermal damage threshold (TDT) line (dose equivalent of 43°C for 2 min) was 93.3% ± 10.6%, and with the blue TDT line (dose equivalent of 43°C for 10 min) was 88.0% ± 14.2%. There were 7 perioperative complications (12%) and 2 mortalities (3.4%). Median overall survival after LITT for the total cohort was 11.5 mo, and median progression-free survival 6.6 mo.
Conclusion: LITT appears to be a safe and effective treatment for GBM in properly selected patients.
Keywords: Brain tumors; GBM; Glioblastoma; LITT; Laser ablation; Laser interstitial thermal therapy; MRI; Thermoablation.
© Congress of Neurological Surgeons 2018.
Figures
References
-
- Stupp R, Mason WP, van den Bent MJ, et al. Radiotherapy plus concomitant and adjuvant temozolomide for glioblastoma. N Engl J Med. 2005;352(10):987–996. - PubMed
-
- Lacroix M, Abi-Said D, Fourney DR, et al. A multivariate analysis of 416 patients with glioblastoma multiforme: prognosis, extent of resection, and survival. J Neurosurg. 2001;95(2):190–198. - PubMed
-
- Sanai N, Polley MY, McDermott MW, Parsa AT, Berger MS. An extent of resection threshold for newly diagnosed glioblastomas. J Neurosurg. 2011;115(1):3–8. - PubMed
-
- Thomas JG, Rao G, Kew Y, Prabhu SS. Laser interstitial thermal therapy for newly diagnosed and recurrent glioblastoma. Neurosurg Focus. 2016;41(4):1–6, E12. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
