

Modeling Health Benefits and Harms of Public Policy Responses to the US Opioid Epidemic
- PMID: 30138057
- PMCID: PMC6137764
- DOI: 10.2105/AJPH.2018.304590
Modeling Health Benefits and Harms of Public Policy Responses to the US Opioid Epidemic
Abstract
Objectives: To estimate health outcomes of policies to mitigate the opioid epidemic.
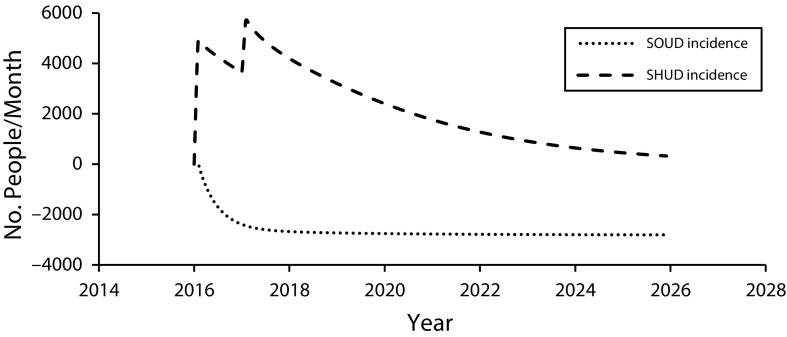
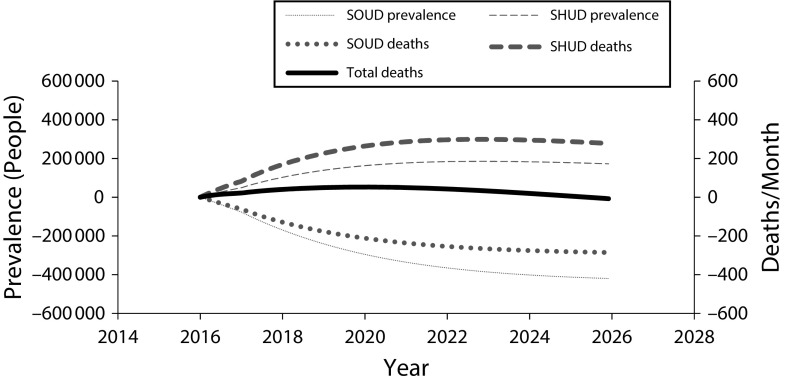
Methods: We used dynamic compartmental modeling of US adults, in various pain, opioid use, and opioid addiction health states, to project addiction-related deaths, life years, and quality-adjusted life years from 2016 to 2025 for 11 policy responses to the opioid epidemic.
Results: Over 5 years, increasing naloxone availability, promoting needle exchange, expanding medication-assisted addiction treatment, and increasing psychosocial treatment increased life years and quality-adjusted life years and reduced deaths. Other policies reduced opioid prescription supply and related deaths but led some addicted prescription users to switch to heroin use, which increased heroin-related deaths. Over a longer horizon, some such policies may avert enough new addiction to outweigh the harms. No single policy is likely to substantially reduce deaths over 5 to 10 years.
Conclusions: Policies focused on services for addicted people improve population health without harming any groups. Policies that reduce the prescription opioid supply may increase heroin use and reduce quality of life in the short term, but in the long term could generate positive health benefits. A portfolio of interventions will be needed for eventual mitigation.
Figures
Comment in
-
We Cannot Treat the Dead.Am J Public Health. 2018 Oct;108(10):1286-1288. doi: 10.2105/AJPH.2018.304658. Am J Public Health. 2018. PMID: 30207778 Free PMC article. No abstract available.
References
-
- Ahmad FB, Rossen LM, Spencer MR, Warner M, Sutton P. Provisional drug overdose death counts. Atlanta, GA: National Center for Health Statistics; 2017.
-
- Krashin D, Sullivan M, Ballantyne J. What are we treating with chronic opioid therapy? Curr Rheumatol Rep. 2013;15(3):311. - PubMed
-
- Lembke A, Humphreys K, Newmark J. Weighing the risks and benefits of chronic opioid therapy. Am Fam Physician. 2016;93(12):982–990. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
