

Risk of intracranial hemorrhage (RICH) in users of oral antithrombotic drugs: Nationwide pharmacoepidemiological study
- PMID: 30138389
- PMCID: PMC6107180
- DOI: 10.1371/journal.pone.0202575
Risk of intracranial hemorrhage (RICH) in users of oral antithrombotic drugs: Nationwide pharmacoepidemiological study
Abstract
Background: The risks of intracranial haemorrhage (ICH) associated with antithrombotic drugs outside clinical trials are gaining increased attention. The aim of this nationwide study was to investigate the risk of ICH requiring hospital admission in users of antithrombotic drugs.
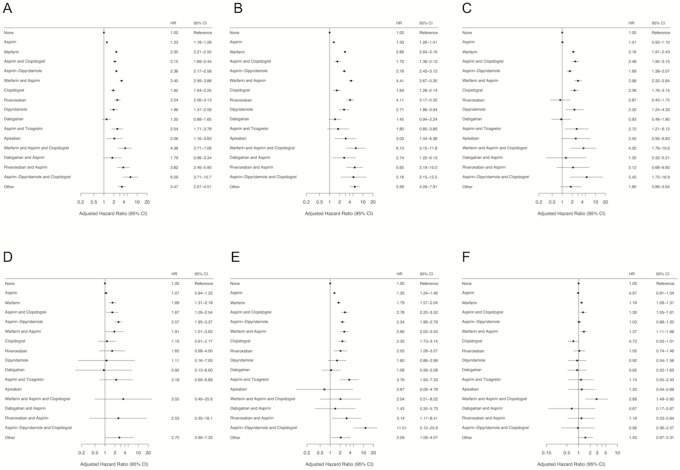
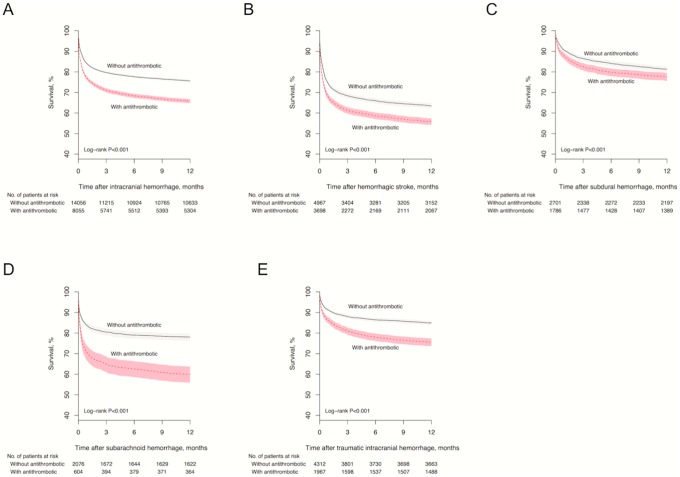
Methods and findings: Data from the Norwegian Patient Registry and Norwegian Prescription Database were linked on an individual level. The primary outcome was incidence rates of ICH associated with use of antithrombotic drugs. Secondary endpoints were risk of ICH and fatal outcome following ICH assessed by Cox models. Among 3,131,270 individuals ≥18 years old observed from 2008 through 2014, there were 729,818 users of antithrombotic medications and 22,111 ICH hospitalizations. Annual crude ICH rates per 100 person-years were 0.076 (95% CI, 0.075-0.077) in non-users and 0.30 (95% CI, 0.30-0.31) in users of antithrombotic medication, with the highest age and sex adjusted rates observed for aspirin-dipyridamole plus clopidogrel (0.44; 95% CI, 0.19-0.69), rivaroxaban plus aspirin (0.36; 95% CI, 0.16-0.56), warfarin plus aspirin (0.34; 95% CI, 0.26-0.43), and warfarin plus aspirin and clopidogrel (0.33; 95% CI, 0.073-0.60). With no antithrombotic medication as reference, the highest adjusted hazard ratios (HR) for ICH were observed for aspirin-dypiridamole plus clopidogrel (6.29; 95% CI 3.71-10.7), warfarin plus aspirin and clopidogrel (4.38; 95% CI 2.71-7.09), rivaroxaban plus aspirin (3.82; 95% CI, 2.46-5.95), and warfarin plus aspirin (3.40; 95% CI, 2.99-3.86). All antithrombotic medication regimens were associated with an increased risk of ICH, except dabigatran monotherapy (HR 1.20; 95% CI, 0.88-1.65) and dabigatran plus aspirin (HR 1.79; 95% CI, 0.96-3.34). Fatal outcome within 90 days was more common in users (2,603 of 8,055) than non-users (3,228 of 14,056) of antithrombotic medication (32.3% vs 23.0%, p<0.001), and was associated with use of warfarin plus aspirin and clopidogrel (HR 2.89; 95% CI, 1.49-5.60), warfarin plus aspirin (HR 1.37; 95% CI, 1.11-1.68), aspirin plus clopidogrel (HR 1.30; 95% CI, 1.05-1.61), and warfarin (HR 1.19; 95% CI, 1.09-1.31). Increased one-year mortality was observed in users of antithrombotic medication following hemorrhagic stroke, subdural hemorrhage, subarachnoid hemorrhage, and traumatic ICH (all p<0.001). Limitations include those inherent to observational studies including the inability to make causal inferences, certain assumptions regarding drug exposure, and the possibility of residual confounding.
Conclusions: The real-world incidence rates and risks of ICH were generally higher than reported in randomized controlled trials. There is still major room for improvement in terms of antithrombotic medication safety (clinicaltrials.gov NCT02481011).
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Sorensen R, Hansen ML, Abildstrom SZ, Hvelplund A, Andersson C, Jorgensen C, et al. Risk of bleeding in patients with acute myocardial infarction treated with different combinations of aspirin, clopidogrel, and vitamin K antagonists in Denmark: a retrospective analysis of nationwide registry data. Lancet. 2009;374(9706):1967–74. Epub 2009/12/17. 10.1016/S0140-6736(09)61751-7 . - DOI - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
