

Screening and management of pre-eclampsia and eclampsia in antenatal and labor and delivery services: findings from cross-sectional observation studies in six sub-Saharan African countries
- PMID: 30139342
- PMCID: PMC6108136
- DOI: 10.1186/s12884-018-1972-1
Screening and management of pre-eclampsia and eclampsia in antenatal and labor and delivery services: findings from cross-sectional observation studies in six sub-Saharan African countries
Abstract
Background: Preeclampsia and eclampsia (PE/E) are major contributors to maternal and neonatal deaths in developing countries, associated with 10-15% of direct maternal deaths and nearly a quarter of stillbirths and newborn deaths, many of which are preventable with improved care. We present results related to WHO-recommended interventions for screening and management of PE/E during antenatal care (ANC) and labor and delivery (L & D) from a study conducted in six sub-Saharan African countries.
Methods: From 2010 to 2012, cross-sectional studies which directly observed provision of ANC and L & D services in six sub-Saharan African countries were conducted. Results from 643 health facilities of different levels in Ethiopia (n = 19), Kenya (n = 509), Madagascar (n = 36), Mozambique (n = 46), Rwanda (n = 72), and Tanzania (n = 52), were combined for this analysis. While studies were sampled separately in each country, all used standardized observation checklists and inventory assessment tools.
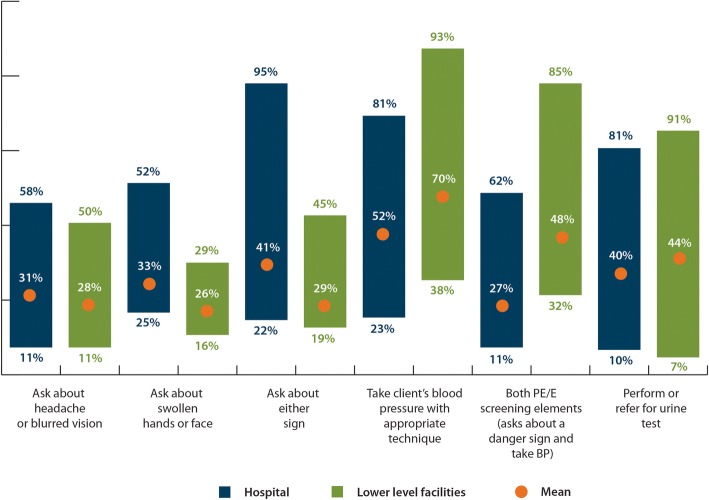
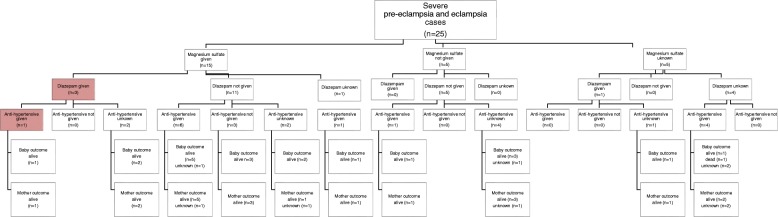
Results: 2920 women receiving ANC and 2689 women in L & D were observed. Thirty-nine percent of ANC clients were asked about PE/E danger signs, and 68% had their blood pressure (BP) taken correctly (range 48-96%). Roughly half (46%) underwent testing for proteinuria. Twenty-three percent of women in L & D were asked about PE/E danger signs (range 11-34%); 77% had their BP checked upon admission (range 59-85%); and 6% had testing for proteinuria. Twenty-five cases of severe PE/E were observed: magnesium sulfate (MgSO4) was used in 15, not used in 5, and for 5 use was unknown. The availability of MgSO4 in L & D varied from 16% in Ethiopia to 100% in Mozambique.
Conclusions: Observed ANC consultations and L & D cases showed low use of WHO-recommended practices for PE/E screening and management. Availability of MgSO4 was low in multiple countries, though it was on the essential drug list of all surveyed countries. Country programs are encouraged to address gaps in screening and management of PE/E in ANC and L & D to contribute to lower maternal and perinatal mortality.
Keywords: Antenatal care; Eclampsia; Ethiopia; Kenya; Labor and delivery; Mozambique; Pre-eclampsia; Quality of care; Rwanda; Tanzania; Zanzibar.
Conflict of interest statement
Ethics approval and consent to participate
The studies were approved by the Institutional Review Board (IRB) of the Johns Hopkins Bloomberg School of Public Health (IRB#00002549) as well as IRBs in each of the participating countries (Tanzania: National Institute of Medical Research [NIMR]; Zanzibar: Zanzibar Research Council [ZRC]; Kenya: Kenya Ministry of Health Institutional Review Board; Mozambique: Mozambican National Ethics Committee, National Institute of Health of Mozambique; Ethiopia: Ethiopian Public Health Association [EPHA]; Rwanda: Rwanda National Ethical Committee [RNEC]; Madagascar: Madagascar Ethical Committee, Ministry of Health of Mozambique). The MACRO International IRB also reviewed the Kenya study, since this was integrated into the national Service Provision Assessment (SPA) conducted by MEASURE DHS. As approved by the respective IRB’s, oral informed consent was obtained from study participants, and documented in data collection tools, prior to data collection.
Consent for publication
Not applicable.
Competing interests
All authors declare no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- WHO. WHO recommendations for Prevention and treatment of pre-eclampsia and eclampsia: Geneva Switzerland; 2011. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
