

Impact of Percutaneous Revascularization on Exercise Hemodynamics in Patients With Stable Coronary Disease
- PMID: 30139442
- PMCID: PMC6580361
- DOI: 10.1016/j.jacc.2018.06.033
Impact of Percutaneous Revascularization on Exercise Hemodynamics in Patients With Stable Coronary Disease
Abstract
Background: Recently, the therapeutic benefits of percutaneous coronary intervention (PCI) have been challenged in patients with stable coronary artery disease (SCD).
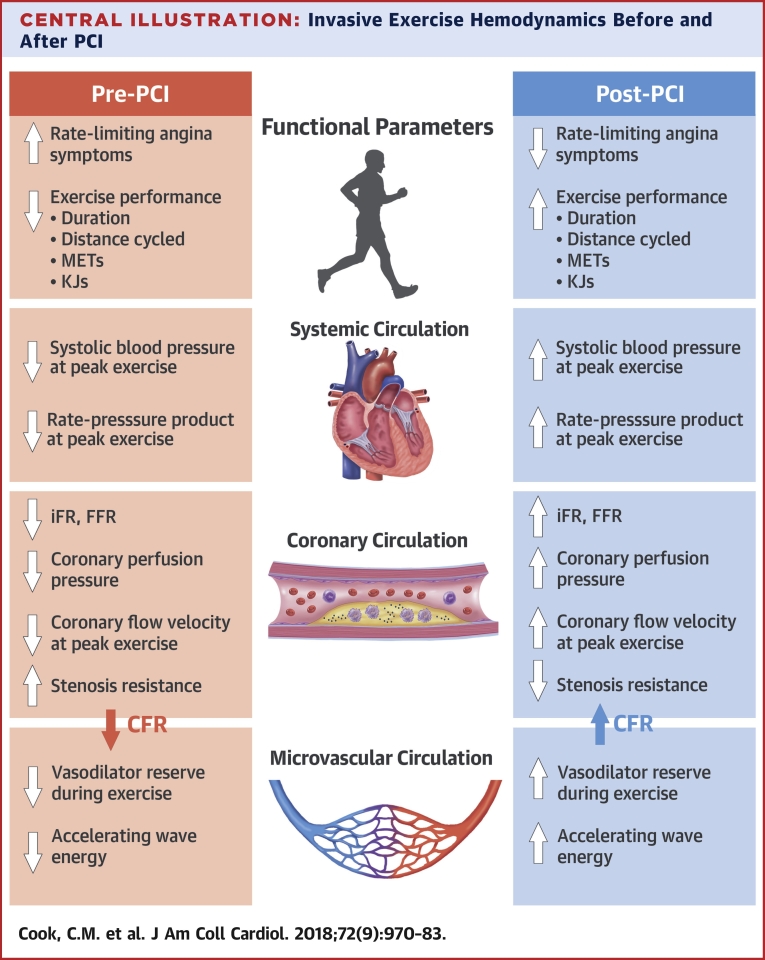
Objectives: The authors examined the impact of PCI on exercise responses in the coronary circulation, the microcirculation, and systemic hemodynamics in patients with SCD.
Methods: A total of 21 patients (mean age 60.3 ± 8.4 years) with SCD and single-vessel coronary stenosis underwent cardiac catheterization. Pre-PCI, patients exercised on a supine ergometer until rate-limiting angina or exhaustion. Simultaneous trans-stenotic coronary pressure-flow measurements were made throughout exercise. Post-PCI, this process was repeated. Physiological parameters, rate-limiting symptoms, and exercise performance were compared between pre-PCI and post-PCI exercise cycles.
Results: PCI reduced ischemia as documented by fractional flow reserve value (pre-PCI 0.59 ± 0.18 to post-PCI 0.91 ± 0.07), instantaneous wave-free ratio value (pre-PCI 0.61 ± 0.27 to post-PCI 0.96 ± 0.05) and coronary flow reserve value (pre-PCI 1.7 ± 0.7 to post-PCI 3.1 ± 1.0; p < 0.001 for all). PCI increased peak-exercise average peak coronary flow velocity (p < 0.0001), coronary perfusion pressure (distal coronary pressure; p < 0.0001), systolic blood pressure (p = 0.01), accelerating wave energy (p < 0.001), and myocardial workload (rate-pressure product; p < 0.01). These changes observed immediately following PCI resulted from the abolition of stenosis resistance (p < 0.0001). PCI was also associated with an immediate improvement in exercise time (+67 s; 95% confidence interval: 31 to 102 s; p < 0.0001) and a reduction in rate-limiting angina symptoms (81% reduction in rate-limiting angina symptoms post-PCI; p < 0.001).
Conclusions: In patients with SCD and severe single-vessel stenosis, objective physiological responses to exercise immediately normalize following PCI. This is seen in the coronary circulation, the microcirculation, and systemic hemodynamics.
Keywords: coronary physiology; exercise; percutaneous coronary intervention; stable coronary disease.
Copyright © 2018 The Authors. Published by Elsevier Inc. All rights reserved.
Figures








Comment in
-
Newsflash, PCI Works: Stenting Stenoses Increases Coronary Blood Flow During Exercise and Reduces Ischemia.J Am Coll Cardiol. 2018 Aug 28;72(9):984-986. doi: 10.1016/j.jacc.2018.06.035. J Am Coll Cardiol. 2018. PMID: 30139443 No abstract available.
References
-
- Al-Lamee R., Thompson D., Dehbi H.-M. Percutaneous coronary intervention in stable angina (ORBITA): a double-blind, randomised controlled trial. Lancet. 2018;391:31–40. - PubMed
-
- Parisi A.F., Folland E.D., Hartigan P. A comparison of angioplasty with medical therapy in the treatment of single-vessel coronary artery disease. N Engl J Med. 1992;326:10–16. - PubMed
-
- Weintraub W.S., Spertus J.A., Kolm P. Effect of PCI on quality of life in patients with stable coronary disease. N Engl J Med. 2008;359:677–687. - PubMed
-
- Wijeysundera H.C., Nallamothu B.K., Krumholz H.M., Tu J.V., Ko D.T. Meta-analysis: effects of percutaneous coronary intervention versus medical therapy on angina relief. Ann Intern Med. 2010;152:370–379. - PubMed
-
- Lockie T.P.E., Rolandi M.C., Guilcher A. Synergistic adaptations to exercise in the systemic and coronary circulations that underlie the warm-up angina phenomenon. Circulation. 2012;126:2565–2574. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
