

Long-term weight change and health outcomes for sleeve gastrectomy (SG) and matched Roux-en-Y gastric bypass (RYGB) participants in the Longitudinal Assessment of Bariatric Surgery (LABS) study
- PMID: 30139560
- PMCID: PMC6594190
- DOI: 10.1016/j.surg.2018.06.008
Long-term weight change and health outcomes for sleeve gastrectomy (SG) and matched Roux-en-Y gastric bypass (RYGB) participants in the Longitudinal Assessment of Bariatric Surgery (LABS) study
Abstract
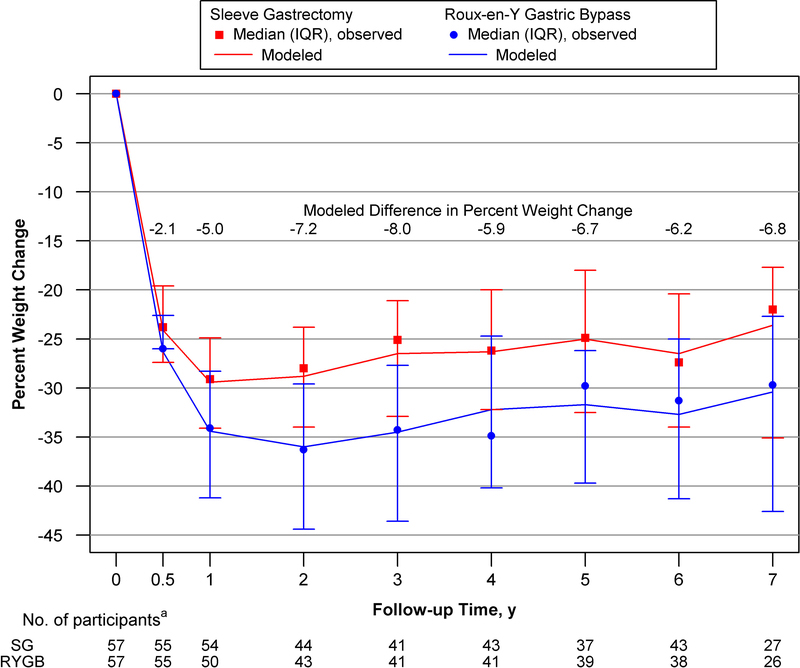
Background: Data from a US multicenter longitudinal study of bariatric surgery were used to compare weight change (primary outcome) and comorbidities (secondary outcome) in patients who underwent sleeve gastrectomy versus Roux-en-Y gastric bypass.
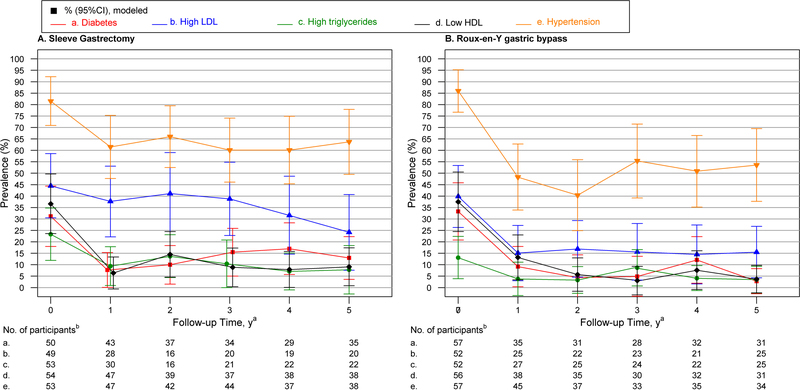
Methods: This study includes participants who underwent sleeve gastrectomy and matched participants who underwent Roux-en-Y gastric bypass from the Longitudinal Assessment of Bariatric Surgery-2 (LABS-2) study. Adults undergoing initial bariatric surgical procedures between 2006 and 2009 were enrolled. Participants who underwent sleeve gastrectomy were high-risk or superobese and intended to have a second-stage procedure. Mixed models were used to evaluate percent weight change from baseline through 7 years, and diabetes, dyslipidemia, and hypertension prevalence through 5 years.
Results: Fifty-seven of 59 participants who underwent sleeve gastrectomy were matched one to one. Most were female (68%) and white (81%), and had a median age of 49 (37-56) years and median body mass index of 56.4 (35.5-76.8) kg/m2 presurgery. Weight loss was significantly less 1 to 7 years after sleeve gastrectomy versus matched Roux-en-Y gastric bypass (eg, year 7 mean weight loss was 23.6% vs 30.4%, respectively; P = .001). For both surgical groups, prevalence of diabetes, low high-density lipoprotein, and hypertension were significantly (P < .05) lower 5 years postsurgery versus baseline.
Conclusion: Higher-risk or super-obese participants after sleeve gastrectomy lost less weight than did matched Roux-en-Y gastric bypass counterparts throughout 7 years. Both groups exhibited improvements in comorbidities from presurgery through 5 years.
Copyright © 2018 Elsevier Inc. All rights reserved.
Conflict of interest statement
CONFLICT OF INTEREST
Dr. Pomp receives speaker honoraria form WL Gore & associates, Ethicon and Medtronics., Drs. King, Belle and Dakin and Ms. Hinerman have nothing to disclose.
Figures
Comment in
-
Discussion.Surgery. 2018 Oct;164(4):782-783. doi: 10.1016/j.surg.2018.06.049. Surgery. 2018. PMID: 30244905 No abstract available.
References
-
- Mechanick JI, Youdim A, Jones DB, Garvey WT, Hurley DL, McMahon MM, et al. Clinical practice guidelines for the perioperative nutritional, metabolic, and nonsurgical support of the bariatric surgery patient−−2013 update: cosponsored by American Association of Clinical Endocrinologists, The Obesity Society, and American Society for Metabolic & Bariatric Surgery. Obesity. 2013;21 Suppl 1:S1–27. - PMC - PubMed
-
- Brethauer SA, Kothari S, Sudan R, Williams B, English WJ, Bregman M, et al. Systematic review on reoperative bariatric surgery American Society for Metabolic and Bariatric Surgery Revision Task Force. SOARD. 2014. - PubMed
-
- Clinical Issues Committee of the American Society for M, Bariatric S. Updated position statement on sleeve gastrectomy as a bariatric procedure. Surgery for obesity and related diseases : official journal of the American Society for Bariatric Surgery. 2010;6(1):1–5. - PubMed
-
- Cottam D, Qureshi FG, Mattar SG, Sharma S, Holover S, Bonanomi G, et al. Laparoscopic sleeve gastrectomy as an initial weight-loss procedure for high-risk patients with morbid obesity. Surg Endosc. 2006;20(6):859–63. - PubMed
-
- Committee ACI. Updated position statement on sleeve gastrectomy as a bariatric procedure. Surgery for obesity and related diseases : official journal of the American Society for Bariatric Surgery. 2012;8(3):e21–6. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
