

Variation in Diagnostic Test Use and Associated Outcomes in Staphylococcal Scalded Skin Syndrome at Children's Hospitals
- PMID: 30139766
- PMCID: PMC6317540
- DOI: 10.1542/hpeds.2018-0032
Variation in Diagnostic Test Use and Associated Outcomes in Staphylococcal Scalded Skin Syndrome at Children's Hospitals
Abstract
Objectives: The incidence of staphylococcal scalded skin syndrome (SSSS) is rising, but current practice variation in diagnostic test use is not well described. Our aim was to describe the variation in diagnostic test use in children hospitalized with SSSS and to determine associations with patient outcomes.
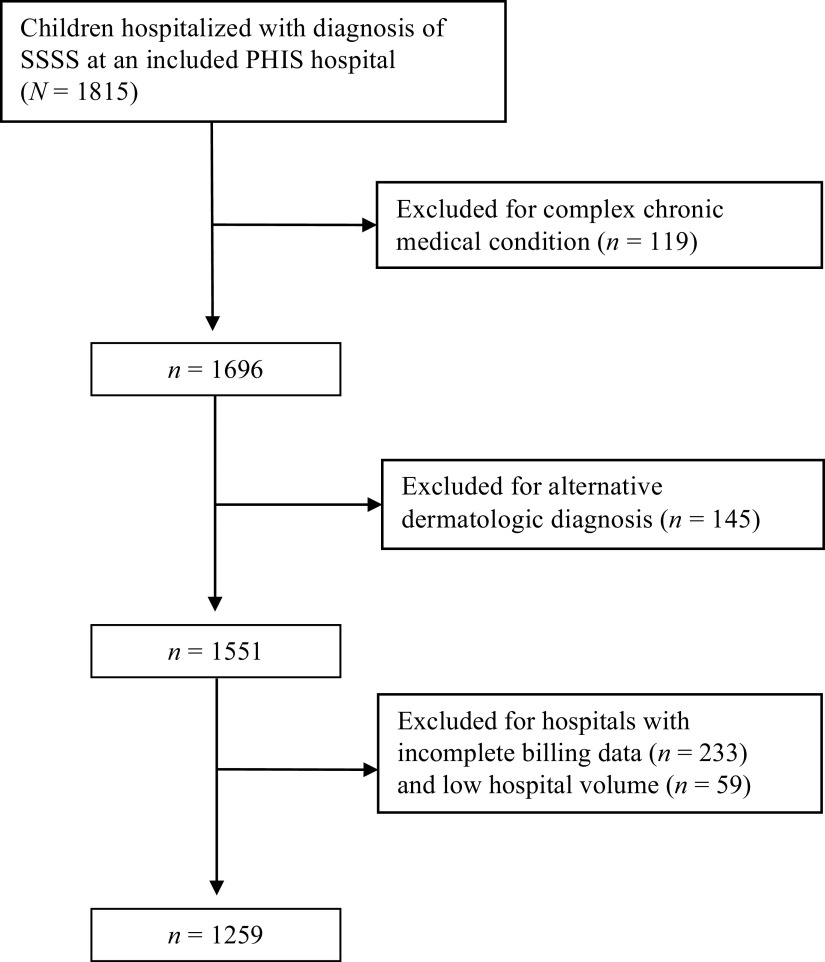
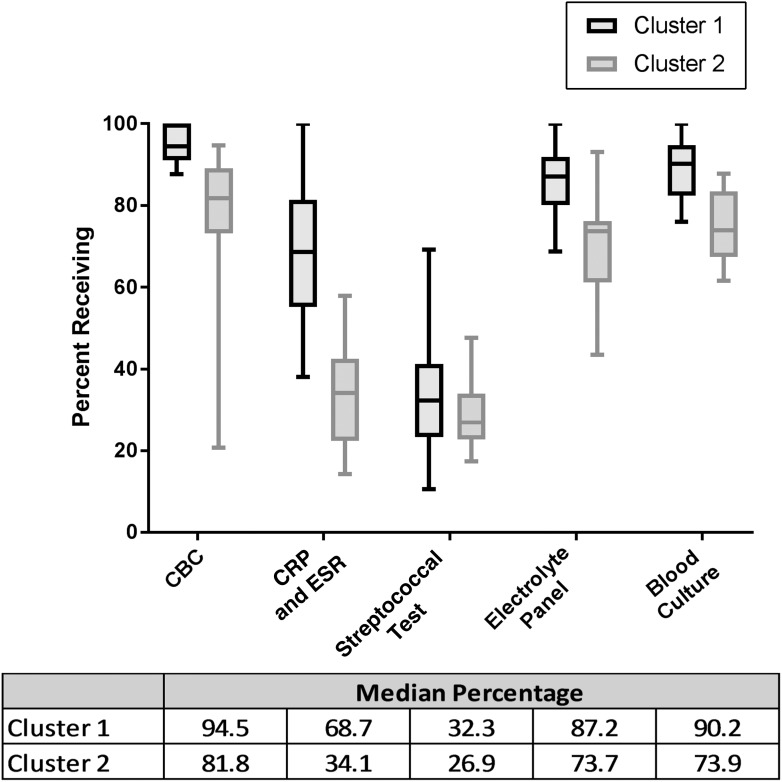
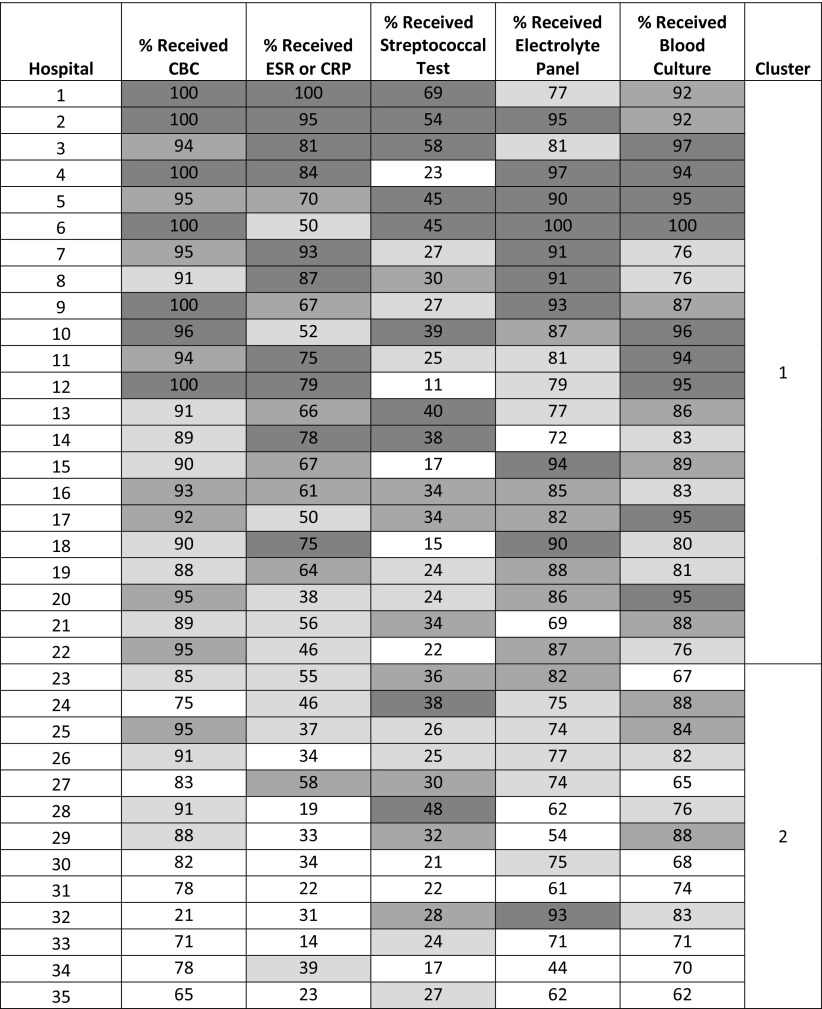
Methods: We performed a retrospective (2011-2016) cohort study of children aged 0 to 18 years from 35 children's hospitals in the Pediatric Health Information System database. Tests included blood culture, complete blood count, erythrocyte sedimentation rate, C-reactive protein level, serum chemistries, and group A streptococcal testing. K-means clustering was used to stratify hospitals into groups of high (cluster 1) and low (cluster 2) test use. Associations between clusters and patient outcomes (length of stay, cost, readmissions, and emergency department revisits) were assessed with generalized linear mixed-effects modeling.
Results: We included 1259 hospitalized children with SSSS; 84% were ≤4 years old. Substantial interhospital variation was seen in diagnostic testing. Blood culture was the most commonly obtained test (range 62%-100%), with the most variation seen in inflammatory markers (14%-100%). Between hospital clusters 1 and 2, respectively, there was no significant difference in adjusted length of stay (2.6 vs 2.5 days; P = .235), cost ($4752 vs $4453; P = .591), same-cause 7-day readmission rate (0.8% vs 0.4%; P = .349), or emergency department revisit rates (0.1% vs 0.6%; P = .148).
Conclusions: For children hospitalized with SSSS, lower use of diagnostic tests was not associated with changes in outcomes. Hospitals with high diagnostic test use may be able to reduce testing without adversely affecting patient outcomes.
Copyright © 2018 by the American Academy of Pediatrics.
Conflict of interest statement
POTENTIAL CONFLICT OF INTEREST: The authors have indicated they have no potential conflicts of interest to disclose.
Figures
References
-
- Lamand V, Dauwalder O, Tristan A, et al. Epidemiological data of staphylococcal scalded skin syndrome in France from 1997 to 2007 and microbiological characteristics of Staphylococcus aureus associated strains. Clin Microbiol Infect. 2012;18(12):E514–E521 - PubMed
-
- Hulten KG, Kok M, King K, Mason EO, Lamberth LB, Kaplan SL. Increasing numbers of staphylococcal scalded skin syndrome cases at Texas Children’s Hospital are caused by ST121. Open Forum Infect Dis. 2016;3(suppl 1):671 - PubMed
-
- Faden H. Neonatal staphylococcal skin infections. Pediatr Infect Dis J. 2003;22(4):389. - PubMed
-
- Li MY, Hua Y, Wei GH, Qiu L. Staphylococcal scalded skin syndrome in neonates: an 8-year retrospective study in a single institution. Pediatr Dermatol. 2014;31(1):43–47 - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
